Tuesday, 31 May 2016
Golden State Warriors' Leandro Barbosa Swears By His Horse Medicine
http://mjm.ag/1q3ZJgm via @MensJournal
When ethical leader behavior breaks bad: How ethical leader behavior can turn abusive via ego depletion and moral licensing.
Lin, Szu-Han (Joanna); Ma, Jingjing; Johnson, Russell E.
Journal of Applied Psychology, Vol 101(6), Jun 2016, 815-830.
http://dx.doi.org/10.1037/apl0000098
Abstract
- The literature to date has predominantly focused on the benefits of ethical leader behaviors for recipients (e.g., employees and teams). Adopting an actor-centric perspective, in this study we examined whether exhibiting ethical leader behaviors may come at some cost to leaders. Drawing from ego depletion and moral licensing theories, we explored the potential challenges of ethical leader behavior for actors. Across 2 studies which employed multiwave designs that tracked behaviors over consecutive days, we found that leaders’ displays of ethical behavior were positively associated with increases in abusive behavior the following day. This association was mediated by increases in depletion and moral credits owing to their earlier displays of ethical behavior. These results suggest that attention is needed to balance the benefits of ethical leader behaviors for recipients against the challenges that such behaviors pose for actors, which include feelings of mental fatigue and psychological license and ultimately abusive interpersonal behaviors. (PsycINFO Database Record (c) 2016 APA, all rights reserved)
When are do-gooders treated badly? Legitimate power, role expectations, and reactions to moral objection in organizations.
Wellman, Ned; Mayer, David M.; Ong, Madeline; DeRue, D. Scott
Journal of Applied Psychology, Vol 101(6), Jun 2016, 793-814.
http://dx.doi.org/10.1037/apl0000094
Abstract
- Organization members who engage in “moral objection” by taking a principled stand against ethically questionable activities help to prevent such activities from persisting. Unfortunately, research suggests that they also may be perceived as less warm (i.e., pleasant, nice) than members who comply with ethically questionable procedures. In this article, we draw on role theory to explore how legitimate power influences observers’ responses to moral objection. We argue that individuals expect those high in legitimate power to engage in moral objection, but expect those low in legitimate power to comply with ethically questionable practices. We further propose that these contrasting role expectations influence the extent to which moral objectors are perceived as warm and subjected to social sanctions (i.e., insults, pressure, unfriendly behavior). We test our predictions with 3 experiments. Study 1, which draws on participants’ prior workplace experiences, supports the first section of our mediated moderation model in which the negative association between an actor’s moral objection (vs. compliance) and observers’ warmth perceptions is weaker when the actor is high rather than low in legitimate power and this effect is mediated by observers’ met role expectations. Study 2, an online experiment featuring a biased hiring task, reveals that the warmth perceptions fostered by the Behavior × Legitimate Power interaction influence observers’ social sanctioning intentions. Finally, Study 3, a laboratory experiment which exposes participants to unethical behavior in a virtual team task, replicates Study 2’s findings and extends the results to actual as well as intended social sanctions. (PsycINFO Database Record (c) 2016 APA, all rights reserved)
Re: Aloe Vera and Chlorine Dioxide Mouth Rinses Reduce Plaque and Gingivitis in Patients with Fixed Orthodontics
| |
| Date: 05-13-2016 | HC# 041621-544 |
Yeturu SK, Acharya S, Urala AS, Pentapati KC. Effect of aloe vera, chlorine dioxide, and chlorhexidine mouth rinses on plaque and gingivitis: a randomized controlled trial. J Oral Biol Craniofac Res. January-April 2016;6(1):54-58.
Dental plaque formation is caused by the presence of bacterial colonies on the teeth and can lead to gingivitis, periodontal disease, and dental caries. Bacteria and plaque can be removed with both mechanical (brushing, flossing, and dental instruments) and chemical (mouthwash) means. However, mechanical cleaning can be particularly difficult in patients with fixed orthodontic hardware and some mouth rinses, while effective, have unwanted side effects, including allergic reactions, mouth lesions, and a disturbance in the sensation of taste. Aloe vera (Aloe vera, Xanthorrhoeaceae) and chlorine dioxide mouth rinses may provide better alternatives to conventional mouth rinses. The mucilaginous gel within the aloe vera leaf has been shown to have antibacterial, antioxidant, and anti-inflammatory properties. Chlorine dioxide is an antibacterial agent and is often used to disinfect the mouth during dental procedures and to treat halitosis and gingivitis. The goal of this randomized, controlled, single-blind study was to measure the efficacy of aloe vera and chlorine dioxide mouth rinses in reducing plaque and gingivitis in dental patients with fixed orthodontic hardware.
The study was conducted at the Department of Orthodontics, Manipal College of Dental Sciences, Manipal University in Manipal, Karnataka, India. Patients were included if they were > 18 years old, had visible plaque and gingivitis associated with > 30% of the teeth examined, and had fixed orthodontics for more than 3 months. Patients were excluded from the study if they had multiple dental restorations or gross dental caries, had used antibiotics during the last 2 weeks, were tobacco (Nicotiana spp., Solanaceae) users, regularly used mouth rinses or antimicrobials, or had removable dental appliances. The extent of plaque and gingivitis was measured with the Silness and Löe Plaque Index and Gingival Index before and after the treatment. Ninety patients were randomly divided into 3 treatment groups—an aloe vera group, a chlorine dioxide group, and a chlorhexidine group. Chlorhexidine was used as the positive control. The sources of the mouth rinses were not provided. Patients were instructed to rinse with 10 ml of mouthwash for 1 minute 2 times per day for a total of 15 days. Data were analyzed with paired t-tests and analysis of variance with post hoc Dunnett's tests.
Five patients were lost from the chlorhexidine group due to non-compliance with the protocol. Plaque and gingivitis were significantly reduced in all of the treatment groups (P < 0.001 for all). There was a significant treatment effect on plaque and gingivitis reduction (P = 0.03 and 0.04, respectively). The percent mean reduction of plaque for aloe vera, chlorine dioxide, and chlorhexidine was 20.38, 30.29, and 31.59, respectively; a similar trend was seen in percent mean reduction of gingivitis of 9.88, 12.22, and 16.30, respectively.
Aloe vera and chlorine dioxide mouth rinses both significantly reduced plaque and gingivitis in dental patients with fixed orthodontics. Chlorine dioxide was nearly as effective as chlorhexidine in reducing plaque and gingivitis. Aloe vera was not as effective as chlorhexidine or chlorine dioxide in reducing plaque and gingivitis, but still resulted in a significant decrease in these measures. The study may have been limited by the small sample size. In addition, the concentrations and sources of the mouth rinses were not given, making it difficult to understand the phytochemical composition of the aloe vera used and to compare these results with results from similar studies.
—Cheryl McCutchan, PhD
Re: Guayusa (Ilex guayusa) Extract Is Nontoxic in Rodent Studies and In Vitro Assays
Kapp RW Jr, Mendes O, Roy S, McQuate RS, Kraska R. General and genetic toxicology of guayusa concentrate (Ilex guayusa). Int J Toxicol. 2016;35(2):222-242.
Guayusa (Ilex guayusa, Aquifoliaceae) is a close relative of yerba maté (Ilex paraguariensis) and is traditionally consumed as a tea or as chewed leaves in the Amazonian region. Guayusa has been found to contain active compounds known as methylxanthines, including caffeine, known to have cellular and systemic stimulatory activity. Data on the safety and adverse effects of guayusa are limited. This study investigated its safety profile using in vitro and in vivo studies with a concentrated water extract of guayusa (procured from Runa LLC; Quito, Ecuador).
Guayusa concentrate (GC) was prepared by brewing leaves in hot water as for tea, at a per weight ratio of 1.3 to 1.6:1 for two to four hours. In vitro, the Ames test was used to gauge mutagenic activity. Briefly, this assay measures genetic mutations in Salmonella typhimurium and Escherichia coli. Water was used as a negative control and several known mutagenic compounds, such as sodium azide, were employed as positive controls. GC concentrations of 1.58, 5.0, 15.8, 50, 158, 500, 1580, and 5000 µg/plate were used, and mutation factor (MF) was calculated as the ratio of mutations observed in the test group to those in the control group (MF of 2 or 3, depending upon the strain, is considered mutagenic). A second in vitro test used to gauge GC toxicity was the chromosomal aberration assay. Human peripheral blood lymphocytes were incubated with GC for four and 20 hours, and for four hours with GC and a metabolic activation system mix; two compounds known to induce chromosomal aberration were used as positive controls, and pure caffeine was tested for comparison.
Three in vivo tests, both acute and long term, in rats also were conducted. To determine acute toxicity, female rats between eight and nine weeks old, said to be more sensitive than males, were studied. GC was administered orally by gavage at 5000 mg/kg to a single rat. When death did not occur, the same dosage was given to two other rats. As no mortality occurred, this study was stopped. Animals were observed daily for 14 days following the GC ingestion and weighed on days seven and 14; they were then sacrificed and necropsies were conducted. To determine dosages for a 90-day study, a 14-day study was conducted in 70 rats (both male and female) at six to seven weeks old, divided into seven treatment arms, each with five males and five females. Treatments included a distilled water control, three GC dosages (1200, 2500, and 5000 mg/kg/day), and three caffeine dosages comparable to the caffeine content in the GC dosages (36, 75, and 150 mg/kg/day). Caffeine dosages were determined based on expected caffeine content of 3% in GC; all treatments were given by gavage at 10 ml/kg. Weights and food consumption were recorded at baseline and on days three, seven, 11, and 14 of the study. Animals were euthanized on day 15. During this experiment, dosing samples were assessed on days one, seven, and 14 for caffeine and chlorogenic acid content to confirm stability of the preparation.
For the 90-day in vivo experiment, GC dosages of 0, 1200, 2500, and 5000 mg/kg/day and a single caffeine dose of 150 mg/kg/day (the amount in the 5000 mg/kg/day GC dosage) were chosen. This experiment used 100 rats, both male and female, at eight weeks of age. At baseline and day 81, rats' eyes were screened. General health was assessed daily and weekly, with weights and food consumption measured throughout the experiment. At day 86 or 87, urine and blood samples were taken. At the end of the study, animals were euthanized, and necropsy and histological analysis were conducted. Dosing samples and the original GC lot were tested for stability on days one, 43, and 94.
Chemical characterization of the main lot of GC detected caffeine at 36 mg/ml, chlorogenic acids at 52 mg/ml, and small amounts of several catechins and theobromine. GC was also analyzed for the presence of a number of major plant compounds (e.g., delphinidins, beta-sitosterol, genistein) that were not found. The extract was found to be adequately stable, and actual caffeine dosages given in all studies were within 15% of the expected amounts. In the Ames test, no problems such as toxicity, precipitation, or contamination were seen. The MF did not increase significantly in any strain at any dose level, so it was determined that GC is not mutagenic. Also, neither GC nor dose-equivalent concentrations of caffeine caused chromosomal aberrations in the chromosomal aberration assay.
In the acute toxicity study, rats were hypoactive and displayed salivation, respiratory, and fecal abnormalities, and hunched posture. At day three, these adverse effects were gone, and the animals remained healthy through day 14. It was concluded that the oral median lethal dose (LD50) of GC is > 5000 mg/kg body weight for female rats. In the 14-day experiment, no death was observed. Hypoactivity and salivation were seen in animals given 5000 mg/kg/day of GC and 75 or 150 mg/kg/day of caffeine. In general, weight loss and decreased food intake occurred in animals consuming either GC or caffeine. This effect disappeared during the course of the study. Necropsy did not show any abnormalities associated with GC or caffeine.
During the 90-day in vivo study, no deaths linked to GC treatment were reported. Three animals died during the study of what were believed to be unrelated causes (though exact cause of death could not be determined) and one was sacrificed due to ill health caused by a dental problem. Hypoactivity and salivation were noted in some animals taking either GC or caffeine. No animals showed any ocular changes. Across the study, weight and food efficiency declined in treated groups, but nonsignificantly. According to the histology, weights of fat pads and several organs in both males and females of the GC and caffeine groups were significantly decreased as compared to control animals, and hypertrophy of salivary glands was observed. Urine composition was unchanged in male rats, with unimportant reduction in protein content in female rats in the high-dose GC and caffeine groups. Small, dose-dependent changes in blood measurements (hemoglobin, red blood cell distribution width, and others) in females, decreased blood triglycerides, and increased cholesterol and liver function enzymes were noted in rats on both GC and caffeine. The authors review previous literature reporting most of these biological effects to result from caffeine consumption.
Overall, this study reports that GC does not show toxicity in the assays and animals employed here. Adverse effects noted at high doses were most likely due to the caffeine content of GC, as caffeine was tested alongside the botanical and caused similar adverse effects. Clarifying the ideal dosage and adverse effects in a clinical setting is worthy of further study.
This study was financially supported by Runa LLC. Three of the authors (RW Kapp Jr, R. Kraska, and RS McQuate) are independent consultants to Runa LLC.
—Amy C. Keller, PhD
Re: Ginger Aromatherapy Improves Some Quality-of-Life Parameters for Patients with Breast Cancer Suffering from Chemotherapy-induced Nausea and Vomiting
| |
| Date: 05-31-2016 | HC# 101554-545 |
Lua PL, Salihah N, Mazlan N. Effects of inhaled ginger aromatherapy on chemotherapy-induced nausea and vomiting and health-related quality of life in women with breast cancer. Complement Ther Med. 2015;23(3):396-404.
Nausea and vomiting are troublesome adverse effects of breast cancer chemotherapy which may negatively affect both patient compliance and quality of life. Ginger (Zingiber officinale, Zingiberaceae) rhizome is used orally to treat nausea; however, it may cause heartburn, diarrhea, and mouth irritation. The authors hypothesized that ginger aromatherapy may prevent chemotherapy-induced nausea and vomiting (CINV) without the potential side effects of oral ginger. Hence, the purpose of this single-blind, randomized, crossover study was to evaluate the effect of aromatherapy with ginger essential oil in alleviating CINV in patients with breast cancer undergoing chemotherapy.
Patients (n = 75; mean age, 47 years) were recruited from December 2011 to January 2014 from oncology clinics at Hospital Sultanah Nur Zahirah in Kuala Terengganu, Terengganu, Malaysia, and Hospital Raja Perempuan Zainab II in Kota Bharu, Kelantan, Malaysia. Included patients had a normal sense of smell, were receiving chemotherapy for breast cancer, had ≥ 2 chemotherapy courses remaining, and had nausea and/or vomiting of any severity. Patients were excluded if they had any other type of cancer; were allergic to ginger, perfumes, or cosmetics; or were undergoing concurrent radiotherapy. All patients received standard CINV drugs for 6 days. In addition, they wore an aromatherapy necklace with a small bottle pendant day and night for 5 days during the period of chemotherapy (the authors do not explain why the aromatherapy was not administered for 6 days as well). The necklace pendant was 20 cm from their nose. At least 3x/day for at least 2 min, patients held the pendant just under their nose and breathed in deeply, even if they were not experiencing symptoms.
The aromatherapy pendant contained 2 drops of either ginger essential oil or placebo ginger fragrance oil (both from Take It Global Sdn Bhd; Butterworth, Penang, Malaysia). "While ginger essential oil is a naturally-occurring substance found in ginger rhizome, the fragrance oil (placebo) is a blend of aroma components that contains ginger oil extract (a concentrated product) and synthetic materials (typically the esters, aldehydes and ketones of various aromatics). Basically, both oils were identical in appearance and texture but the therapeutic values of fragrance oil may have decreased substantially due to changes in the chemical structure of the concentrated product (extract) and mixture of synthetic components." After approximately a 2-week washout (average time between chemotherapy sessions) when the necklace was not worn, patients switched to the opposite treatment. Severity of nausea was measured with a visual analog scale. Incidence of vomiting was recorded. Health-related quality of life (HRQoL) was assessed with the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30) at baseline and 8 days postchemotherapy. The authors do not explain why HRQoL was not assessed at the end of the aromatherapy.
A total of 60 patients completed all study visits and were included in the analysis. The majority of patients (66.6%) were in early stages of disease (stages I and II), and 86.7% of patients received highly emetogenic (having the capacity to induce vomiting) chemotherapy. There were no significant differences between groups at baseline. Blinding was 93.3% effective, with only 4 patients in each group reporting they could detect a difference between the treatments. Compliance was not reported.
There was no significant difference between groups in severity of nausea or incidence of vomiting. However, the ginger essential oil group had a significant reduction in severity of nausea over time, with the greatest effect in alleviating acute nausea on day 1 (P = 0.040). In regard to the HRQoL scores, there was a significant improvement from baseline with ginger essential oil in global health status (P < 0.001), role functioning (P = 0.002), fatigue (P = 0.001), pain (P = 0.013), nausea and vomiting (P < 0.001), appetite loss (P < 0.001), and constipation (P < 0.040). The degree of improvement in role functioning and appetite loss met the criteria for clinically relevant change (10-point variation from baseline score). No major adverse effects were reported; 1 patient withdrew due to mild dizziness on day 5 of ginger essential oil aromatherapy.
In the discussion, the authors note several points for consideration. The episodes of vomiting were low across all time points, so it is possible that the frequency of vomiting was not high enough to detect a therapeutic effect. Secondly, studies have shown that patients who have previously undergone chemotherapy are more likely to experience CINV and have increased resistance to antiemetics. The patients who received the placebo treatment first may have developed increased resistance before crossing over to the ginger treatment. In addition, the highly emetogenic chemotherapy used in this trial is associated with delayed symptoms which are less responsive to treatment. And while there were limited improvements in the objective measures, the HRQoL scores suggest that even relatively small reductions in CINV severity may translate to significant improvement in subjective outcome measures. An acknowledged limitation of the study was that the severity of nausea and vomiting before enrollment was not measured and was assumed to be equal across the groups. Also, it is possible that the "placebo" ginger fragrance had some therapeutic benefit.
The authors conclude that ginger essential oil had limited effects in reducing CINV; however, the HRQoL findings "were … encouraging with significant improvement in several domains." They recommend that future studies include an untreated control arm (aromatherapy placebo such as water) to give a more accurate comparison and assessment of the placebo effect.
—Heather S. Oliff, PhD
Neoliberalism: Oversold?
https://shar.es/1dTVaK via @sharethis
Finance & Development, June 2016, Vol. 53, No. 2
 Instead of delivering growth, some neoliberal policies have increased inequality, in turn jeopardizing durable expansion
Instead of delivering growth, some neoliberal policies have increased inequality, in turn jeopardizing durable expansion
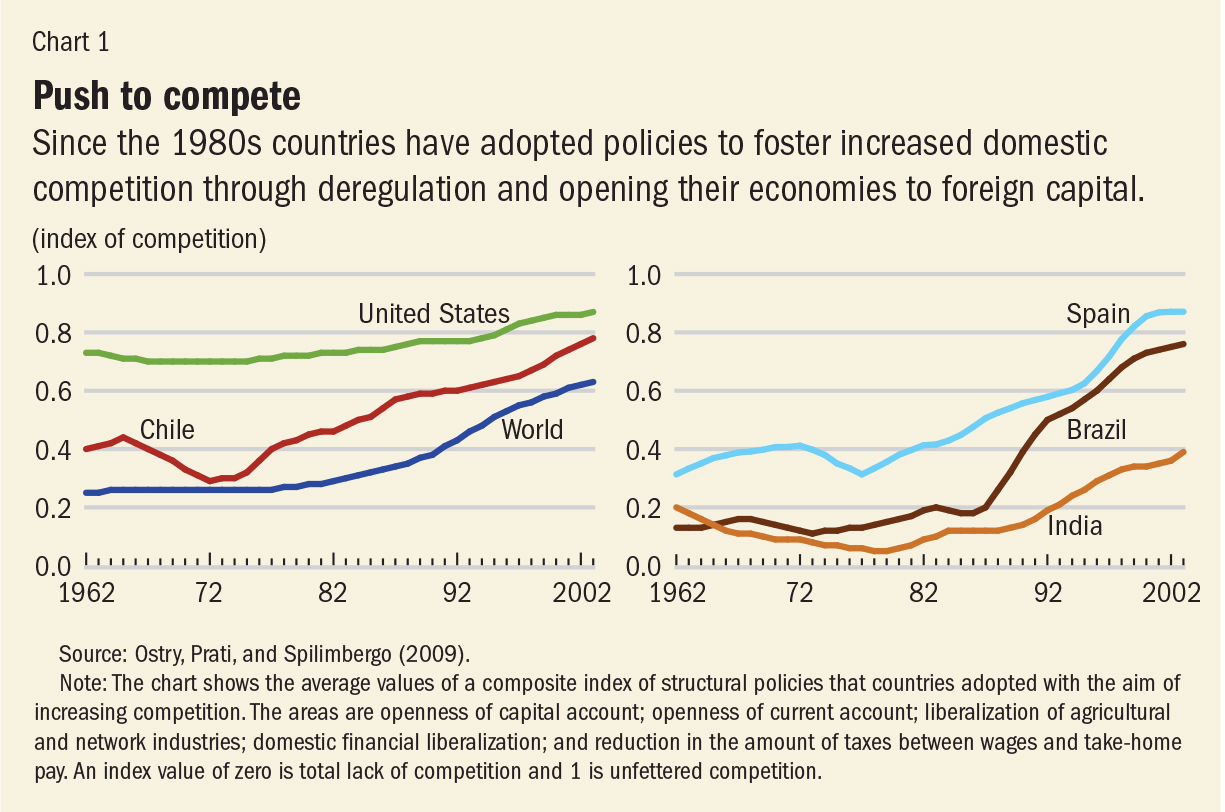
Milton Friedman in 1982 hailed Chile as an “economic miracle.” Nearly a decade earlier, Chile had turned to policies that have since been widely emulated across the globe. The neoliberal agenda—a label used more by critics than by the architects of the policies—rests on two main planks. The first is increased competition—achieved through deregulation and the opening up of domestic markets, including financial markets, to foreign competition. The second is a smaller role for the state, achieved through privatization and limits on the ability of governments to run fiscal deficits and accumulate debt.
There has been a strong and widespread global trend toward neoliberalism since the 1980s, according to a composite index that measures the extent to which countries introduced competition in various spheres of economic activity to foster economic growth. As shown in the left panel of Chart 1, Chile’s push started a decade or so earlier than 1982, with subsequent policy changes bringing it ever closer to the United States. Other countries have also steadily implemented neoliberal policies (see Chart 1, right panel).
 There is much to cheer in the neoliberal agenda. The expansion of
global trade has rescued millions from abject poverty. Foreign direct
investment has often been a way to transfer technology and know-how to
developing economies. Privatization of state-owned enterprises has in
many instances led to more efficient provision of services and lowered
the fiscal burden on governments.
There is much to cheer in the neoliberal agenda. The expansion of
global trade has rescued millions from abject poverty. Foreign direct
investment has often been a way to transfer technology and know-how to
developing economies. Privatization of state-owned enterprises has in
many instances led to more efficient provision of services and lowered
the fiscal burden on governments.
However, there are aspects of the neoliberal agenda that have not delivered as expected. Our assessment of the agenda is confined to the effects of two policies: removing restrictions on the movement of capital across a country’s borders (so-called capital account liberalization); and fiscal consolidation, sometimes called “austerity,” which is shorthand for policies to reduce fiscal deficits and debt levels. An assessment of these specific policies (rather than the broad neoliberal agenda) reaches three disquieting conclusions:
•The benefits in terms of increased growth seem fairly difficult to establish when looking at a broad group of countries.
•The costs in terms of increased inequality are prominent. Such costs epitomize the trade-off between the growth and equity effects of some aspects of the neoliberal agenda.
•Increased inequality in turn hurts the level and sustainability of growth. Even if growth is the sole or main purpose of the neoliberal agenda, advocates of that agenda still need to pay attention to the distributional effects.
This indeed turns out to be the case. The link between financial openness and economic growth is complex. Some capital inflows, such as foreign direct investment—which may include a transfer of technology or human capital—do seem to boost long-term growth. But the impact of other flows—such as portfolio investment and banking and especially hot, or speculative, debt inflows—seem neither to boost growth nor allow the country to better share risks with its trading partners (Dell’Ariccia and others, 2008; Ostry, Prati, and Spilimbergo, 2009). This suggests that the growth and risk-sharing benefits of capital flows depend on which type of flow is being considered; it may also depend on the nature of supporting institutions and policies.
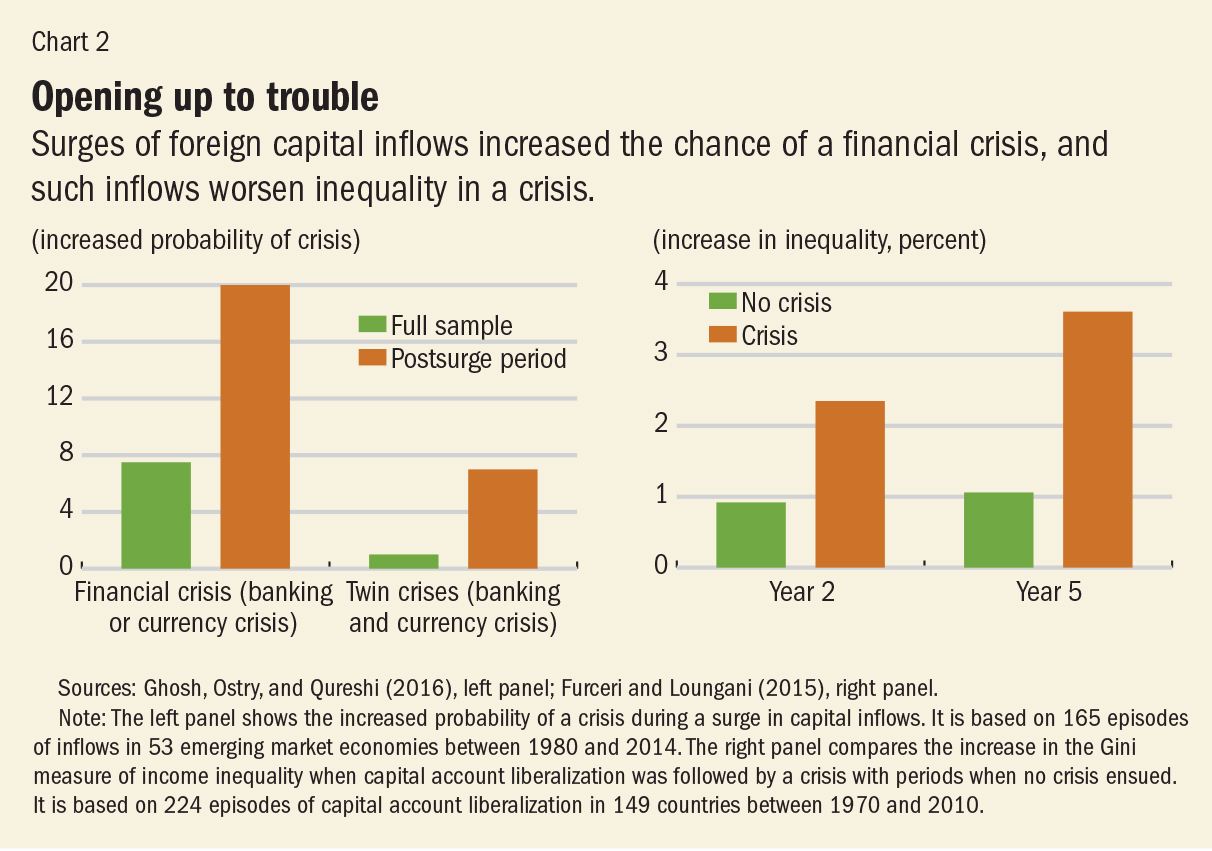
Although growth benefits are uncertain, costs in terms of increased economic volatility and crisis frequency seem more evident. Since 1980, there have been about 150 episodes of surges in capital inflows in more than 50 emerging market economies; as shown in the left panel of Chart 2, about 20 percent of the time, these episodes end in a financial crisis, and many of these crises are associated with large output declines (Ghosh, Ostry, and Qureshi, 2016).
 The pervasiveness of booms and busts gives credence to the claim by
Harvard economist Dani Rodrik that these “are hardly a sideshow or a
minor blemish in international capital flows; they are the main story.”
While there are many drivers, increased capital account openness
consistently figures as a risk factor in these cycles. In addition to
raising the odds of a crash, financial openness has distributional
effects, appreciably raising inequality (see Furceri and Loungani, 2015,
for a discussion of the channels through which this operates).
Moreover, the effects of openness on inequality are much higher when a
crash ensues (Chart 2, right panel).
The pervasiveness of booms and busts gives credence to the claim by
Harvard economist Dani Rodrik that these “are hardly a sideshow or a
minor blemish in international capital flows; they are the main story.”
While there are many drivers, increased capital account openness
consistently figures as a risk factor in these cycles. In addition to
raising the odds of a crash, financial openness has distributional
effects, appreciably raising inequality (see Furceri and Loungani, 2015,
for a discussion of the channels through which this operates).
Moreover, the effects of openness on inequality are much higher when a
crash ensues (Chart 2, right panel).
The mounting evidence on the high cost-to-benefit ratio of capital account openness, particularly with respect to short-term flows, led the IMF’s former First Deputy Managing Director, Stanley Fischer, now the vice chair of the U.S. Federal Reserve Board, to exclaim recently: “What useful purpose is served by short-term international capital flows?” Among policymakers today, there is increased acceptance of controls to limit short-term debt flows that are viewed as likely to lead to—or compound—a financial crisis. While not the only tool available—exchange rate and financial policies can also help—capital controls are a viable, and sometimes the only, option when the source of an unsustainable credit boom is direct borrowing from abroad (Ostry and others, 2012).
Economic theory provides little guidance on the optimal public debt target. Some theories justify higher levels of debt (since taxation is distortionary) and others point to lower—or even negative—levels (since adverse shocks call for precautionary saving). In some of its fiscal policy advice, the IMF has been concerned mainly with the pace at which governments reduce deficits and debt levels following the buildup of debt in advanced economies induced by the global financial crisis: too slow would unnerve markets; too fast would derail recovery. But the IMF has also argued for paying down debt ratios in the medium term in a broad mix of advanced and emerging market countries, mainly as insurance against future shocks.
But is there really a defensible case for countries like Germany, the United Kingdom, or the United States to pay down the public debt? Two arguments are usually made in support of paying down the debt in countries with ample fiscal space—that is, in countries where there is little real prospect of a fiscal crisis. The first is that, although large adverse shocks such as the Great Depression of the 1930s or the global financial crisis of the past decade occur rarely, when they do, it is helpful to have used the quiet times to pay down the debt. The second argument rests on the notion that high debt is bad for growth—and, therefore, to lay a firm foundation for growth, paying down the debt is essential.
It is surely the case that many countries (such as those in southern Europe) have little choice but to engage in fiscal consolidation, because markets will not allow them to continue borrowing. But the need for consolidation in some countries does not mean all countries—at least in this case, caution about “one size fits all” seems completely warranted. Markets generally attach very low probabilities of a debt crisis to countries that have a strong record of being fiscally responsible (Mendoza and Ostry, 2007). Such a track record gives them latitude to decide not to raise taxes or cut productive spending when the debt level is high (Ostry and others, 2010; Ghosh and others, 2013). And for countries with a strong track record, the benefit of debt reduction, in terms of insurance against a future fiscal crisis, turns out to be remarkably small, even at very high levels of debt to GDP. For example, moving from a debt ratio of 120 percent of GDP to 100 percent of GDP over a few years buys the country very little in terms of reduced crisis risk (Baldacci and others, 2011).
But even if the insurance benefit is small, it may still be worth incurring if the cost is sufficiently low. It turns out, however, that the cost could be large—much larger than the benefit. The reason is that, to get to a lower debt level, taxes that distort economic behavior need to be raised temporarily or productive spending needs to be cut—or both. The costs of the tax increases or expenditure cuts required to bring down the debt may be much larger than the reduced crisis risk engendered by the lower debt (Ostry, Ghosh, and Espinoza, 2015). This is not to deny that high debt is bad for growth and welfare. It is. But the key point is that the welfare cost from the higher debt (the so-called burden of the debt) is one that has already been incurred and cannot be recovered; it is a sunk cost. Faced with a choice between living with the higher debt—allowing the debt ratio to decline organically through growth—or deliberately running budgetary surpluses to reduce the debt, governments with ample fiscal space will do better by living with the debt.
Austerity policies not only generate substantial welfare costs due to supply-side channels, they also hurt demand—and thus worsen employment and unemployment. The notion that fiscal consolidations can be expansionary (that is, raise output and employment), in part by raising private sector confidence and investment, has been championed by, among others, Harvard economist Alberto Alesina in the academic world and by former European Central Bank President Jean-Claude Trichet in the policy arena. However, in practice, episodes of fiscal consolidation have been followed, on average, by drops rather than by expansions in output. On average, a consolidation of 1 percent of GDP increases the long-term unemployment rate by 0.6 percentage point and raises by 1.5 percent within five years the Gini measure of income inequality (Ball and others, 2013).
In sum, the benefits of some policies that are an important part of the neoliberal agenda appear to have been somewhat overplayed. In the case of financial openness, some capital flows, such as foreign direct investment, do appear to confer the benefits claimed for them. But for others, particularly short-term capital flows, the benefits to growth are difficult to reap, whereas the risks, in terms of greater volatility and increased risk of crisis, loom large.
In the case of fiscal consolidation, the short-run costs in terms of lower output and welfare and higher unemployment have been underplayed, and the desirability for countries with ample fiscal space of simply living with high debt and allowing debt ratios to decline organically through growth is underappreciated.
The evidence of the economic damage from inequality suggests that policymakers should be more open to redistribution than they are. Of course, apart from redistribution, policies could be designed to mitigate some of the impacts in advance—for instance, through increased spending on education and training, which expands equality of opportunity (so-called predistribution policies). And fiscal consolidation strategies—when they are needed—could be designed to minimize the adverse impact on low-income groups. But in some cases, the untoward distributional consequences will have to be remedied after they occur by using taxes and government spending to redistribute income. Fortunately, the fear that such policies will themselves necessarily hurt growth is unfounded (Ostry, 2014).
For example, its former chief economist, Olivier Blanchard, said in 2010 that “what is needed in many advanced economies is a credible medium-term fiscal consolidation, not a fiscal noose today.” Three years later, IMF Managing Director Christine Lagarde said the institution believed that the U.S. Congress was right to raise the country’s debt ceiling “because the point is not to contract the economy by slashing spending brutally now as recovery is picking up.” And in 2015 the IMF advised that countries in the euro area “with fiscal space should use it to support investment.”
On capital account liberalization, the IMF’s view has also changed—from one that considered capital controls as almost always counterproductive to greater acceptance of controls to deal with the volatility of capital flows. The IMF also recognizes that full capital flow liberalization is not always an appropriate end-goal, and that further liberalization is more beneficial and less risky if countries have reached certain thresholds of financial and institutional development.
Chile’s pioneering experience with neoliberalism received high praise from Nobel laureate Friedman, but many economists have now come around to the more nuanced view expressed by Columbia University professor Joseph Stiglitz (himself a Nobel laureate) that Chile “is an example of a success of combining markets with appropriate regulation” (2002). Stiglitz noted that in the early years of its move to neoliberalism, Chile imposed “controls on the inflows of capital, so they wouldn’t be inundated,” as, for example, the first Asian-crisis country, Thailand, was a decade and a half later. Chile’s experience (the country now eschews capital controls), and that of other countries, suggests that no fixed agenda delivers good outcomes for all countries for all times. Policymakers, and institutions like the IMF that advise them, must be guided not by faith, but by evidence of what has worked. ■
Ball, Laurence, Davide Furceri, Daniel Leigh, and Prakash Loungani, 2013, “The Distributional Effects of Fiscal Austerity,” UN-DESA Working Paper 129 (New York: United Nations).
Dell’Ariccia, Giovanni, Julian di Giovanni, André Faria, M. Ayhan Kose, Paolo Mauro, Jonathan D. Ostry, Martin Schindler, and Marco Terrones, 2008, Reaping the Benefits of Financial Globalization, IMF Occasional Paper 264 (Washington: International Monetary Fund).
Furceri, Davide, and Prakash Loungani, 2015, “Capital Account Liberalization and Inequality,” IMF Working Paper 15/243 (Washington: International Monetary Fund).
Ghosh, Atish R., Jun I. Kim, Enrique G. Mendoza, Jonathan D. Ostry, and Mahvash S. Qureshi, 2013, “Fiscal Fatigue, Fiscal Space and Debt Sustainability in Advanced Economies,” Economic Journal, Vol. 123, No. 566, pp. F4–F30.
Ghosh, Atish R., Jonathan D. Ostry, and Mahvash S. Qureshi, 2016, “When Do Capital Inflow Surges End in Tears?” American Economic Review, Vol. 106, No. 5.
Mendoza, Enrique G., and Jonathan D. Ostry, 2007, “International Evidence on Fiscal Solvency: Is Fiscal Policy ‘Responsible’?” Journal of Monetary Economics, Vol. 55, No. 6, pp. 1081–93.
Obstfeld, Maurice, 1998, “The Global Capital Market: Benefactor or Menace?” Journal of Economic Perspectives, Vol. 12, No. 4, pp. 9–30.
Ostry, Jonathan D., 2014, “We Do Not Have to Live with the Scourge of Inequality,” Financial Times, March 3.
———, Andrew Berg, and Charalambos Tsangarides, 2014, “Redistribution, Inequality, and Growth,” IMF Staff Discussion Note 14/02 (Washington: International Monetary Fund).
Ostry, Jonathan D., Atish R. Ghosh, Marcos Chamon, and Mahvash S. Qureshi, 2012, “Tools for Managing Financial-Stability Risks from Capital Inflows,” Journal of International Economics, Vol. 88, No. 2, pp. 407–21.
Ostry, Jonathan D., Atish R. Ghosh, Jun I. Kim, and Mahvash Qureshi, 2010, “Fiscal Space,” IMF Staff Position Note 10/11 (Washington: International Monetary Fund).
Ostry, Jonathan D., Atish R. Ghosh, and Raphael Espinoza, 2015, “When Should Public Debt Be Reduced?” IMF Staff Discussion Note 15/10 (Washington: International Monetary Fund).
Ostry, Jonathan D., Alessandro Prati, and Antonio Spilimbergo, 2009, Structural Reforms and Economic Performance in Advanced and Developing Countries, IMF Occasional Paper 268 (Washington: International Monetary Fund).
Rodrik, Dani, 1998, “Who Needs Capital-Account Convertibility?” in Should the IMF Pursue Capital-Account Convertibility? Essays in International Finance 207 (Princeton, New Jersey: Princeton University).
Stiglitz, Joseph, 2002, “The Chilean Miracle: Combining Markets with Appropriate Reform,” Commanding Heights interview.
Instead of delivering growth, some neoliberal policies have increased inequality, in turn jeopardizing durable expansionMilton Friedman in 1982 hailed Chile as an “economic miracle.” Nearly a decade earlier, Chile had turned to policies that have since been widely emulated across the globe. The neoliberal agenda—a label used more by critics than by the architects of the policies—rests on two main planks. The first is increased competition—achieved through deregulation and the opening up of domestic markets, including financial markets, to foreign competition. The second is a smaller role for the state, achieved through privatization and limits on the ability of governments to run fiscal deficits and accumulate debt.
There has been a strong and widespread global trend toward neoliberalism since the 1980s, according to a composite index that measures the extent to which countries introduced competition in various spheres of economic activity to foster economic growth. As shown in the left panel of Chart 1, Chile’s push started a decade or so earlier than 1982, with subsequent policy changes bringing it ever closer to the United States. Other countries have also steadily implemented neoliberal policies (see Chart 1, right panel).
 There is much to cheer in the neoliberal agenda. The expansion of
global trade has rescued millions from abject poverty. Foreign direct
investment has often been a way to transfer technology and know-how to
developing economies. Privatization of state-owned enterprises has in
many instances led to more efficient provision of services and lowered
the fiscal burden on governments.
There is much to cheer in the neoliberal agenda. The expansion of
global trade has rescued millions from abject poverty. Foreign direct
investment has often been a way to transfer technology and know-how to
developing economies. Privatization of state-owned enterprises has in
many instances led to more efficient provision of services and lowered
the fiscal burden on governments.However, there are aspects of the neoliberal agenda that have not delivered as expected. Our assessment of the agenda is confined to the effects of two policies: removing restrictions on the movement of capital across a country’s borders (so-called capital account liberalization); and fiscal consolidation, sometimes called “austerity,” which is shorthand for policies to reduce fiscal deficits and debt levels. An assessment of these specific policies (rather than the broad neoliberal agenda) reaches three disquieting conclusions:
•The benefits in terms of increased growth seem fairly difficult to establish when looking at a broad group of countries.
•The costs in terms of increased inequality are prominent. Such costs epitomize the trade-off between the growth and equity effects of some aspects of the neoliberal agenda.
•Increased inequality in turn hurts the level and sustainability of growth. Even if growth is the sole or main purpose of the neoliberal agenda, advocates of that agenda still need to pay attention to the distributional effects.
Open and shut?
As Maurice Obstfeld (1998) has noted, “economic theory leaves no doubt about the potential advantages” of capital account liberalization, which is also sometimes called financial openness. It can allow the international capital market to channel world savings to their most productive uses across the globe. Developing economies with little capital can borrow to finance investment, thereby promoting their economic growth without requiring sharp increases in their own saving. But Obstfeld also pointed to the “genuine hazards” of openness to foreign financial flows and concluded that “this duality of benefits and risks is inescapable in the real world.”This indeed turns out to be the case. The link between financial openness and economic growth is complex. Some capital inflows, such as foreign direct investment—which may include a transfer of technology or human capital—do seem to boost long-term growth. But the impact of other flows—such as portfolio investment and banking and especially hot, or speculative, debt inflows—seem neither to boost growth nor allow the country to better share risks with its trading partners (Dell’Ariccia and others, 2008; Ostry, Prati, and Spilimbergo, 2009). This suggests that the growth and risk-sharing benefits of capital flows depend on which type of flow is being considered; it may also depend on the nature of supporting institutions and policies.
Although growth benefits are uncertain, costs in terms of increased economic volatility and crisis frequency seem more evident. Since 1980, there have been about 150 episodes of surges in capital inflows in more than 50 emerging market economies; as shown in the left panel of Chart 2, about 20 percent of the time, these episodes end in a financial crisis, and many of these crises are associated with large output declines (Ghosh, Ostry, and Qureshi, 2016).
 The pervasiveness of booms and busts gives credence to the claim by
Harvard economist Dani Rodrik that these “are hardly a sideshow or a
minor blemish in international capital flows; they are the main story.”
While there are many drivers, increased capital account openness
consistently figures as a risk factor in these cycles. In addition to
raising the odds of a crash, financial openness has distributional
effects, appreciably raising inequality (see Furceri and Loungani, 2015,
for a discussion of the channels through which this operates).
Moreover, the effects of openness on inequality are much higher when a
crash ensues (Chart 2, right panel).
The pervasiveness of booms and busts gives credence to the claim by
Harvard economist Dani Rodrik that these “are hardly a sideshow or a
minor blemish in international capital flows; they are the main story.”
While there are many drivers, increased capital account openness
consistently figures as a risk factor in these cycles. In addition to
raising the odds of a crash, financial openness has distributional
effects, appreciably raising inequality (see Furceri and Loungani, 2015,
for a discussion of the channels through which this operates).
Moreover, the effects of openness on inequality are much higher when a
crash ensues (Chart 2, right panel).The mounting evidence on the high cost-to-benefit ratio of capital account openness, particularly with respect to short-term flows, led the IMF’s former First Deputy Managing Director, Stanley Fischer, now the vice chair of the U.S. Federal Reserve Board, to exclaim recently: “What useful purpose is served by short-term international capital flows?” Among policymakers today, there is increased acceptance of controls to limit short-term debt flows that are viewed as likely to lead to—or compound—a financial crisis. While not the only tool available—exchange rate and financial policies can also help—capital controls are a viable, and sometimes the only, option when the source of an unsustainable credit boom is direct borrowing from abroad (Ostry and others, 2012).
Size of the state
Curbing the size of the state is another aspect of the neoliberal agenda. Privatization of some government functions is one way to achieve this. Another is to constrain government spending through limits on the size of fiscal deficits and on the ability of governments to accumulate debt. The economic history of recent decades offers many examples of such curbs, such as the limit of 60 percent of GDP set for countries to join the euro area (one of the so-called Maastricht criteria).Economic theory provides little guidance on the optimal public debt target. Some theories justify higher levels of debt (since taxation is distortionary) and others point to lower—or even negative—levels (since adverse shocks call for precautionary saving). In some of its fiscal policy advice, the IMF has been concerned mainly with the pace at which governments reduce deficits and debt levels following the buildup of debt in advanced economies induced by the global financial crisis: too slow would unnerve markets; too fast would derail recovery. But the IMF has also argued for paying down debt ratios in the medium term in a broad mix of advanced and emerging market countries, mainly as insurance against future shocks.
But is there really a defensible case for countries like Germany, the United Kingdom, or the United States to pay down the public debt? Two arguments are usually made in support of paying down the debt in countries with ample fiscal space—that is, in countries where there is little real prospect of a fiscal crisis. The first is that, although large adverse shocks such as the Great Depression of the 1930s or the global financial crisis of the past decade occur rarely, when they do, it is helpful to have used the quiet times to pay down the debt. The second argument rests on the notion that high debt is bad for growth—and, therefore, to lay a firm foundation for growth, paying down the debt is essential.
It is surely the case that many countries (such as those in southern Europe) have little choice but to engage in fiscal consolidation, because markets will not allow them to continue borrowing. But the need for consolidation in some countries does not mean all countries—at least in this case, caution about “one size fits all” seems completely warranted. Markets generally attach very low probabilities of a debt crisis to countries that have a strong record of being fiscally responsible (Mendoza and Ostry, 2007). Such a track record gives them latitude to decide not to raise taxes or cut productive spending when the debt level is high (Ostry and others, 2010; Ghosh and others, 2013). And for countries with a strong track record, the benefit of debt reduction, in terms of insurance against a future fiscal crisis, turns out to be remarkably small, even at very high levels of debt to GDP. For example, moving from a debt ratio of 120 percent of GDP to 100 percent of GDP over a few years buys the country very little in terms of reduced crisis risk (Baldacci and others, 2011).
But even if the insurance benefit is small, it may still be worth incurring if the cost is sufficiently low. It turns out, however, that the cost could be large—much larger than the benefit. The reason is that, to get to a lower debt level, taxes that distort economic behavior need to be raised temporarily or productive spending needs to be cut—or both. The costs of the tax increases or expenditure cuts required to bring down the debt may be much larger than the reduced crisis risk engendered by the lower debt (Ostry, Ghosh, and Espinoza, 2015). This is not to deny that high debt is bad for growth and welfare. It is. But the key point is that the welfare cost from the higher debt (the so-called burden of the debt) is one that has already been incurred and cannot be recovered; it is a sunk cost. Faced with a choice between living with the higher debt—allowing the debt ratio to decline organically through growth—or deliberately running budgetary surpluses to reduce the debt, governments with ample fiscal space will do better by living with the debt.
Austerity policies not only generate substantial welfare costs due to supply-side channels, they also hurt demand—and thus worsen employment and unemployment. The notion that fiscal consolidations can be expansionary (that is, raise output and employment), in part by raising private sector confidence and investment, has been championed by, among others, Harvard economist Alberto Alesina in the academic world and by former European Central Bank President Jean-Claude Trichet in the policy arena. However, in practice, episodes of fiscal consolidation have been followed, on average, by drops rather than by expansions in output. On average, a consolidation of 1 percent of GDP increases the long-term unemployment rate by 0.6 percentage point and raises by 1.5 percent within five years the Gini measure of income inequality (Ball and others, 2013).
In sum, the benefits of some policies that are an important part of the neoliberal agenda appear to have been somewhat overplayed. In the case of financial openness, some capital flows, such as foreign direct investment, do appear to confer the benefits claimed for them. But for others, particularly short-term capital flows, the benefits to growth are difficult to reap, whereas the risks, in terms of greater volatility and increased risk of crisis, loom large.
In the case of fiscal consolidation, the short-run costs in terms of lower output and welfare and higher unemployment have been underplayed, and the desirability for countries with ample fiscal space of simply living with high debt and allowing debt ratios to decline organically through growth is underappreciated.
An adverse loop
Moreover, since both openness and austerity are associated with increasing income inequality, this distributional effect sets up an adverse feedback loop. The increase in inequality engendered by financial openness and austerity might itself undercut growth, the very thing that the neoliberal agenda is intent on boosting. There is now strong evidence that inequality can significantly lower both the level and the durability of growth (Ostry, Berg, and Tsangarides, 2014).The evidence of the economic damage from inequality suggests that policymakers should be more open to redistribution than they are. Of course, apart from redistribution, policies could be designed to mitigate some of the impacts in advance—for instance, through increased spending on education and training, which expands equality of opportunity (so-called predistribution policies). And fiscal consolidation strategies—when they are needed—could be designed to minimize the adverse impact on low-income groups. But in some cases, the untoward distributional consequences will have to be remedied after they occur by using taxes and government spending to redistribute income. Fortunately, the fear that such policies will themselves necessarily hurt growth is unfounded (Ostry, 2014).
Finding the balance
These findings suggest a need for a more nuanced view of what the neoliberal agenda is likely to be able to achieve. The IMF, which oversees the international monetary system, has been at the forefront of this reconsideration.For example, its former chief economist, Olivier Blanchard, said in 2010 that “what is needed in many advanced economies is a credible medium-term fiscal consolidation, not a fiscal noose today.” Three years later, IMF Managing Director Christine Lagarde said the institution believed that the U.S. Congress was right to raise the country’s debt ceiling “because the point is not to contract the economy by slashing spending brutally now as recovery is picking up.” And in 2015 the IMF advised that countries in the euro area “with fiscal space should use it to support investment.”
On capital account liberalization, the IMF’s view has also changed—from one that considered capital controls as almost always counterproductive to greater acceptance of controls to deal with the volatility of capital flows. The IMF also recognizes that full capital flow liberalization is not always an appropriate end-goal, and that further liberalization is more beneficial and less risky if countries have reached certain thresholds of financial and institutional development.
Chile’s pioneering experience with neoliberalism received high praise from Nobel laureate Friedman, but many economists have now come around to the more nuanced view expressed by Columbia University professor Joseph Stiglitz (himself a Nobel laureate) that Chile “is an example of a success of combining markets with appropriate regulation” (2002). Stiglitz noted that in the early years of its move to neoliberalism, Chile imposed “controls on the inflows of capital, so they wouldn’t be inundated,” as, for example, the first Asian-crisis country, Thailand, was a decade and a half later. Chile’s experience (the country now eschews capital controls), and that of other countries, suggests that no fixed agenda delivers good outcomes for all countries for all times. Policymakers, and institutions like the IMF that advise them, must be guided not by faith, but by evidence of what has worked. ■
Jonathan D. Ostry is a Deputy Director, Prakash Loungani is a Division Chief, and Davide Furceri is an Economist, all in the IMF’s Research Department.
References
Baldacci, Emanuele, Iva Petrova, Nazim Belhocine, Gabriela Dobrescu, and Samah Mazraani, 2011, “Assessing Fiscal Stress,” IMF Working Paper 11/100 (Washington: International Monetary Fund).Ball, Laurence, Davide Furceri, Daniel Leigh, and Prakash Loungani, 2013, “The Distributional Effects of Fiscal Austerity,” UN-DESA Working Paper 129 (New York: United Nations).
Dell’Ariccia, Giovanni, Julian di Giovanni, André Faria, M. Ayhan Kose, Paolo Mauro, Jonathan D. Ostry, Martin Schindler, and Marco Terrones, 2008, Reaping the Benefits of Financial Globalization, IMF Occasional Paper 264 (Washington: International Monetary Fund).
Furceri, Davide, and Prakash Loungani, 2015, “Capital Account Liberalization and Inequality,” IMF Working Paper 15/243 (Washington: International Monetary Fund).
Ghosh, Atish R., Jun I. Kim, Enrique G. Mendoza, Jonathan D. Ostry, and Mahvash S. Qureshi, 2013, “Fiscal Fatigue, Fiscal Space and Debt Sustainability in Advanced Economies,” Economic Journal, Vol. 123, No. 566, pp. F4–F30.
Ghosh, Atish R., Jonathan D. Ostry, and Mahvash S. Qureshi, 2016, “When Do Capital Inflow Surges End in Tears?” American Economic Review, Vol. 106, No. 5.
Mendoza, Enrique G., and Jonathan D. Ostry, 2007, “International Evidence on Fiscal Solvency: Is Fiscal Policy ‘Responsible’?” Journal of Monetary Economics, Vol. 55, No. 6, pp. 1081–93.
Obstfeld, Maurice, 1998, “The Global Capital Market: Benefactor or Menace?” Journal of Economic Perspectives, Vol. 12, No. 4, pp. 9–30.
Ostry, Jonathan D., 2014, “We Do Not Have to Live with the Scourge of Inequality,” Financial Times, March 3.
———, Andrew Berg, and Charalambos Tsangarides, 2014, “Redistribution, Inequality, and Growth,” IMF Staff Discussion Note 14/02 (Washington: International Monetary Fund).
Ostry, Jonathan D., Atish R. Ghosh, Marcos Chamon, and Mahvash S. Qureshi, 2012, “Tools for Managing Financial-Stability Risks from Capital Inflows,” Journal of International Economics, Vol. 88, No. 2, pp. 407–21.
Ostry, Jonathan D., Atish R. Ghosh, Jun I. Kim, and Mahvash Qureshi, 2010, “Fiscal Space,” IMF Staff Position Note 10/11 (Washington: International Monetary Fund).
Ostry, Jonathan D., Atish R. Ghosh, and Raphael Espinoza, 2015, “When Should Public Debt Be Reduced?” IMF Staff Discussion Note 15/10 (Washington: International Monetary Fund).
Ostry, Jonathan D., Alessandro Prati, and Antonio Spilimbergo, 2009, Structural Reforms and Economic Performance in Advanced and Developing Countries, IMF Occasional Paper 268 (Washington: International Monetary Fund).
Rodrik, Dani, 1998, “Who Needs Capital-Account Convertibility?” in Should the IMF Pursue Capital-Account Convertibility? Essays in International Finance 207 (Princeton, New Jersey: Princeton University).
Stiglitz, Joseph, 2002, “The Chilean Miracle: Combining Markets with Appropriate Reform,” Commanding Heights interview.
A feminist encounters two French-speaking men
Recently I was living in situation A where I met a neighbour of French origin. He gossiped about the wife of another neighbour. Gossip is a turnoff for me even though the sociologists say it is necessary, but I gave him a pass because he is helpful with the neighbours. I encountered him a couple more times in which he was helping the neighbour in situation B, where I had moved.
Initially I was alone in situation B except for a few days and then a crew of young men moved in and an older man from Quebec who spent his adult life in the Yukon, Within a day Mr. Quebec was touching me, asking me my life plans and questioning me in a way that I found intrusive. The tasks that I had done on my own suddenly had to be done in pairs and the owner who had tons of stuff to do was suddenly working with me in a basic task. Because the tasks were so basic the sexism that suddenly altered my ability to work hit me really hard. A crew shift for a new task was delayed and I had to grab the chance of a forklift blocking Mr. Quebec's view of me to climb to the new task and change the other members of the crew myself. Within days I was shouting at Mr. Quebec and a few days later I was telling the owners that what they saw as charm I saw as manipulation and I started searching for a new situation. So dear Canada, you are not post-feminist in certain pockets of the population.
Before I left situation B, the French man and his crew invited our crew over for pizza. I sat silently while the French man told a newly arrived female member of his crew that he had a PhD in History, with tops marks, that his mother was one of the top historians in France and that he had run away from his new Ivy league post because he did not want to deal with his mother's reputation.
So I thought - that is interesting from a feminist point of view. His mother seemingly has it all - a successful career and a son she could be proud of, but the son says he cannot handle her success in his own career, even though he moved away from Europe. But as part of his story the French man said he had mild autism. So I thought maybe it is the autism talking and not the sexism talking. Since I was silent I decided to look up his PhD so I would have something to talk about if we met again. I only knew his nickname and Googling his nickname and organic did not work. Then I remembered I had seen small children sitting on his horses. So I Googled his name with horse riding lessons. His triple-C name came up as a member of a drama club, complete with pictures. A 2007 post giving his whearabouts was the first red flag. I thought - if that was his level of English when he accepted the Ivy league post, no wonder he ran away.
I searched his triple-C name using Science Direct - no matches. I thought - Science Direct does not have everything but WorldCat does. WorldCat had no matches. Either the French man does not have a PhD with the name he is using in Canada or he does not have one at all. Or I missed it somehow. But his story about his inability to deal with the career of his successful mother in his own career still seems like a researchable feminist topic.
Initially I was alone in situation B except for a few days and then a crew of young men moved in and an older man from Quebec who spent his adult life in the Yukon, Within a day Mr. Quebec was touching me, asking me my life plans and questioning me in a way that I found intrusive. The tasks that I had done on my own suddenly had to be done in pairs and the owner who had tons of stuff to do was suddenly working with me in a basic task. Because the tasks were so basic the sexism that suddenly altered my ability to work hit me really hard. A crew shift for a new task was delayed and I had to grab the chance of a forklift blocking Mr. Quebec's view of me to climb to the new task and change the other members of the crew myself. Within days I was shouting at Mr. Quebec and a few days later I was telling the owners that what they saw as charm I saw as manipulation and I started searching for a new situation. So dear Canada, you are not post-feminist in certain pockets of the population.
Before I left situation B, the French man and his crew invited our crew over for pizza. I sat silently while the French man told a newly arrived female member of his crew that he had a PhD in History, with tops marks, that his mother was one of the top historians in France and that he had run away from his new Ivy league post because he did not want to deal with his mother's reputation.
So I thought - that is interesting from a feminist point of view. His mother seemingly has it all - a successful career and a son she could be proud of, but the son says he cannot handle her success in his own career, even though he moved away from Europe. But as part of his story the French man said he had mild autism. So I thought maybe it is the autism talking and not the sexism talking. Since I was silent I decided to look up his PhD so I would have something to talk about if we met again. I only knew his nickname and Googling his nickname and organic did not work. Then I remembered I had seen small children sitting on his horses. So I Googled his name with horse riding lessons. His triple-C name came up as a member of a drama club, complete with pictures. A 2007 post giving his whearabouts was the first red flag. I thought - if that was his level of English when he accepted the Ivy league post, no wonder he ran away.
I searched his triple-C name using Science Direct - no matches. I thought - Science Direct does not have everything but WorldCat does. WorldCat had no matches. Either the French man does not have a PhD with the name he is using in Canada or he does not have one at all. Or I missed it somehow. But his story about his inability to deal with the career of his successful mother in his own career still seems like a researchable feminist topic.
Britain's timid university lecturer strike will change nothing in a rigged system
http://rabble.ca/blogs/bloggers/raluca-bejan/2016/05/britains-timid-university-lecturer-protest-will-change-nothing-r?utm_source=feedburner&utm_medium=feed&utm_campaign=Feed%3A+rabble-news+%28rabble.ca+-+News+for+the+rest+of+us%29#.V02bqH88aQc.twitter
How much does tax avoidance damage the public good? Even more than you think.
http://www.policynote.ca/how-much-does-tax-avoidance-damage-the-public-good-even-more-than-you-think/#.V02bZ9ZUx1U.twitter
Coffee and metabolic impairment: An updated review of epidemiological studies
Volume 3, August 2016, Pages 1–7

Open Access
Review article
Coffee and metabolic impairment: An updated review of epidemiological studies
- Under a Creative Commons license
Abstract
Background
Coffee
is one of the most consumed beverages worldwide. In the last years,
coffee consumption has been associated with a number of beneficial
effects against metabolic impairment. The aim of this narrative review
was to report the most updated and comprehensive evidence from
epidemiological and experimental studies as well as mechanisms of action
of coffee on metabolic impairment.
Methods
A
search in electronic databases (PUBMED and EMBASE) was performed to
retrieve systematic and pooled analyses on coffee and diabetes,
hypertension, and dyslipidemia. Furthermore, the most accredited
hypotheses and mechanisms of action of coffee have been described.
Results
Coffee
consumption has been associated with reduced risk of diabetes in
observational studies. However, the effect seems not to be mediated by
caffeine. Contrasting results have been found in pooled analyses of
observational studies on hypertension, despite short- and long-term
follow-ups that have been demonstrated to influence the outcome. Poor or
little effect on plasma lipids has been reported in studies on acute
administration of coffee, yet depending on the type of coffee
preparation. The main beneficial effects of coffee consumption seem to
rely on the content of antioxidant and anti-inflammatory compounds
(i.e., polyphenols). Among the most important, chlorogenic acids have
demonstrated direct anti-hypertensive action through beneficial effect
on endothelial function, and significant improvement in glucose and
insulin metabolism. Also, diterpenes and melanoidins are major
candidates as antioxidant compounds showing the capacity to inhibit the
production of inflammatory mediators. However, caffeine and diterpenes
may also exert negative effects, such as acute rise in blood pressure
and serum lipids.
Conclusion
In
light of the most recent evidence, coffee consumption seems to be
favorably related with health and to protect by metabolic impairment.
Keywords
- Coffee;
- Caffeine;
- Metabolic disorders;
- Diabetes
1. Introduction
Metabolic
disorders, such as obesity, dysregulated glucose homeostasis,
dyslipidemia, and abnormal elevation of systolic and diastolic blood
pressure are important risk factors for cardiovascular disease (CVD) and
are among the major contributors for overall mortality [1].
Overweight and obese population have rapidly increased worldwide
leading to a concomitant rise of type 2 diabetes incidence, especially
in the highest income regions [2].
Hypertension and dyslipidemia affect 20%–40% of the population, showing
a significant association with elevated BMI, waist circumference, and
fasting blood glucose [3].
Altogether, these conditions represent a major public health issue that
could potentially be reduced by the adoption of a healthier lifestyle.
Besides well-known risk factors, such as sedentary and smoking habits,
dietary habits show a crucial impact toward metabolic disorders. Several
investigations pointed out the important role of certain dietary
patterns, such as the Mediterranean diet or the Dietary Approach to Stop
Hypertension (DASH), as significant protective factors against
metabolic disorders and CVD risk factors [4], [5], [6] and [7]. Cohort studies demonstrated positive effects of these dietary patterns in both Mediterranean and non-Mediterranean countries [8] and [9].
However, their application in non-Mediterranean areas is somehow
limited and some important foods have not been taken into account when
considering such dietary patterns. In the last ten years, research on
coffee drinking has increased dramatically suggesting that coffee
consumption is not as negative as it was hypothesized in earlier studies
[10].
In a recent State-of-the-Art review, a moderate coffee consumption (2
to 3 cups per day) has shown potential benefits on cardiometabolic
disease, cardiovascular health, and all-cause mortality [11]; although in other studies, high coffee consumption (> 4 cups per day) could have adverse effects [12].
The findings recently published pointed out convincing hypotheses on
its beneficial effects in preventing metabolic impairment and laboratory
research on its components provided biological plausibility for its
action [13].
In this narrative review, we report the most important epidemiological
evidence on coffee consumption and metabolic impairment, showing the
inconsistency between epidemiological and experimental studies as a
result of the biological differences between short- versus long-time
consumption. Furthermore, the most accredited hypotheses and mechanisms
of action have been described.
2. Epidemiological versus experimental evidence
2.1. Diabetes mellitus, glucose tolerance, and insulin sensitivity
Two
recent systematic reviews and meta-analyses analyzing the specific
association between coffee (data from 28 studies with information on
1,109,272 participants) [14], and decaffeinated coffee (10 studies, 491,485 participants) [15]
on incidence of type 2 diabetes found a nonlinear dose–response
relationship between coffee intake and subsequent risk of type 2
diabetes, with a decrease of about 8% of risk for every 1 cup/day
increment in coffee intake after adjustment for potential confounding
factors (Table 1).
Since similar results were shown for decaffeinated coffee, it is likely
that the protective effect may exist aside from the influence of
caffeine intake. Another systematic review including 13 cohort studies
with 9473 type 2 diabetes cases and 47,387 participants, found a
reduction in type 2 diabetes incidence in those subjects who consumed 4
or more cups per day compared with less than 2 cups drinkers [16] (Table 1).
Advantage emerged comparing intake of filtered coffee over pot boiled
and decaffeinated coffee over caffeinated coffee. However, by analyzing
single studies reporting inconclusive results, a relation with factors
that could explain such results (i.e., type of coffee or country) could
not be found. In addition to the previous systematic reviews, more
recent observational studies are in line with the hypothesis that coffee
intake may be linked to a lower risk of diabetes [17], [18], [19], [20] and [21], reduced risk of deterioration of glucose metabolism [22] and [23], and insulin resistance [24], [25], [26] and [27].
- Table 1. Characteristics of meta-analysis and systematic review included in this review.
Author Year Number and design of the studies Participants Cases Outcome Exposure Main results and RR (95% CI) Diabetes mellitus, glucose tolerance, and insulin sensitivity Ding et al. [14] 2014 28 PCS 1,109,272 43,335 T2DM incidence 0 coffee cup/d 1 1 coffee cups/d 0.92 (0.90, 0.94) 2 coffee cups/d 0.85 (0.82, 0.88) 3 coffee cups/d 0.79 (0.75, 0.83) 4 coffee cups/d 0.75 (0.71, 0.80) 5 coffee cups/d 0.71 (0.65, 0.79) 6 coffee cups/d 0.67 (0.61, 0.74) Jiang et al. [15] 2014 26 PCS 1,096,647 50,595 T2DM incidence Coffee lowest vs highest 0.71 (0.67, 0.76) 10 PCS 491,485 29,165 T2DM incidence Decaffeinated coffee lowest vs highest 0.79 (0.69, 0.91) 6 PCS 321,960 9302 T2DM incidence Caffeine, lowest Vs highest 0.70 (0.65, 0.75) Whitehead et al. [28] 2013 2 RCTs 53 T1DM individuals N/A Hypoglycemic episodes Caffeine 400–500 mg Increased awareness and decreased duration of hypoglycemic episodes 6 RCTs 73 T2DM individuals N/A Blood glucose and insulin sensitivity Caffeine 200–500 mg Increased blood glucose (16%–28%) and insulin levels (19%–48%). Decreased insulin sensitivity by 14%–37%. 1 RCT 8 GDM individuals N/A Blood glucose and insulin sensitivity Caffeine 200 mg Increased blood glucose (19%) and insulin level (29%) and reduced insulin sensitivity by 18%. Muley et al. [16] 2012 13 PCS 12,47,387 9473 T2DM incidence Coffee T2DM incidence was reduced in subjects who drank 4–6 cups/d and 6–7 cups/d compared with < 2 cups/d drinkers Hypertension Mesas et al. [41] 2011 5 RCTs 85 hypertensive individuals N/A Acute effect on BP Caffeine 200–300 mg) SBP 8.14 mmHg (5.68, 10.61) DBP 5.7 mmHg (4.1, 7.4) 6 RCTs 364 hypertensive individuals N/A Long-term effect on BP Coffee or caffeine No change in BP Zhang et al. [39] 2011 6 PCS 172,567 37,135 Hypertension incidence < 1 coffee cup/d 1 1–3 coffee cups/d 1.09 (1.01, 1.18) 3–5 coffee cups/d 1.07 (0.96, 1.20) > 5 coffee cups/d 1.08 (0.96 ,1.21) Noordzija et al. [42] 2005 16 RTCs 110 N/A BP Coffee SBP 1.22 mmHg (0.52, 1.92) DBP 0.49 mmHg (− 0.06, 1.04) Caffeine SBP 4.16 mmHg (2.13, 6.20) DBP 2.41 mmHg (0.98, 3.84) Caffeine and coffee SBP 2.04 mmHg (1.10, 2.99) DBP 0.73 mmHg (0.14, 1.31) Dyslipidemia and lipid metabolism Cai et al. [54] 2012 12 RCT 1017 N/A Serum lipids Coffee 2.4 to 8.0 cups/day TC 8.05 mg/dl (4.48,11.62) LDL-C 5.44 mg/dl (1.38,9.51) HDL-C -0.12 mg/dl (− 0.62, 0.38) TG 12.55 mg/dl (3.47, 21.64) - CI, confidence interval; BP, blood pressure; DBP, diastolic blood pressure; GDM, gestational diabetes mellitus; HDL, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; N/A, not applicable; PCS, prospective cohort study; RTC, randomized controlled trial; SBP, systolic blood pressure; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; TC, total cholesterol; TG, triglyceride.
Generally,
results from randomized controlled trials (RCT) exploring the effect of
coffee consumption on glucose metabolism and biological risk factors
for type 2 diabetes widely contrasted those from observational studies. A
recent meta-analysis of RCT in people with type 2 diabetes reported
substantial negative effect of caffeine intake on blood glucose control [28] (Table 1).
As expected, a major limitation of the trials included in the pooled
analysis was the short period of study. Indeed, the beneficial effects
of caffeinated and decaffeinated instant coffee on glucose metabolism
were found in a recent study that lasted 16 weeks [29],
but studies exploring the acute effects following the meal reported
opposite or inconclusive results. An experimental study conducted on
healthy volunteers resulted in an increasing insulin response and
decreased insulin sensitivity index after a 75 g oral glucose tolerance
test, compared to water [30].
While in another RTC on healthy subjects, coffee consumption increased
glucose concentration and lowered insulin concentrations in the first
30 min after a standardized meal [31].
Caffeinated coffee, after either a high or low glycemic index meal,
significantly impaired acute blood glucose management and insulin
insensitivity compared with ingestion of decaffeinated coffee [32] and [33], despite these effects being stronger after a lipid-rich meal [34].
Moreover, coffee consumption during a carbohydrate meal seems to
decrease the insulin sensitivity of a second carbohydrate meal, even
without an additional coffee intake [35].
Some other experimental studies reported poorly significant results of
caffeinated coffee on postprandial glycemic tolerance and insulin
sensitivity [36] and [37]
or increase of coffee-derived compounds but no changes of markers of
glucose metabolism at an oral glucose tolerance test were found [38].
2.2. Hypertension
Epidemiological
studies exploring the role of coffee consumption on the development of
hypertension showed inconclusive results. Among the several pooled
analysis that have been conducted during last 10 years, the most recent
meta-analysis of epidemiological studies, including 6 prospective
cohorts with a total of 172,567 participants and 37,135 incident cases
of hypertension, concluded that the summary relative risks (RRs) for
hypertension was 1.09 (95% confidence interval (CI): 1.01, 1.18) for
consumption of 1–3 cups per day, whereas no significant risk was found
for higher categories (> 3 cups/day) [39] (Table 1).
A meta-analysis of experimental and observational epidemiological
studies on coffee consumption and hypertension reported low-quality
evidence, unable to show any statistically significant effect of coffee
consumption on blood pressure or the risk of hypertension [40] (Table 1).
Another meta-analysis investigating the role of coffee/caffeine intake
in hypertensive subjects results in an acute increment of BP for ≥ 3,
without any long-term association between coffee intake and BP [41] (Table 1).
These findings seem to confirm the results of a previous meta-analysis
of RCT conducted with regard to the intake of both coffee and caffeine [42] (Table 1).
They reported a significant rise of 2.04 mmHg (95% CI: 1.10, 2.99) in
systolic blood pressure and 0.73 mmHg (95% CI: 0.14, 1.31) in diastolic
blood pressure for pooled analysis of coffee and caffeine trials. When
coffee trials and caffeine trials were analyzed separately, blood
pressure elevations appeared to be significant only for caffeine but not
for coffee, suggesting that despite the biochemical mechanism of action
of caffeine supporting the biological plausibility that acute ingestion
of such compounds may increase blood pressure, when ingested through
coffee, the blood pressure effect of caffeine was somehow attenuated. It
is noteworthy that most recent investigations found a significantly
reduced risk of hypertension evaluated in both cross-sectional and
prospective design only when analysis was stratified by smoking status [43] and [44].
2.3. Dyslipidemia and lipid metabolism
The
early epidemiological studies published in the 1980s demonstrated a
significant association between coffee consumption and increased serum
cholesterol levels [45], [46], [47] and [48].
The hypercholesterolemic effect of coffee has been demonstrated to
depend on the diterpenes cafestol and kahweol, and by the method of
brewing [49].
Contrarily, filtered coffee consumption seems to have poor or no
association with serum lipid levels compared to boiled coffee, maybe due
to the retention of diterpenes by the paper filter [50].
Thus, results from epidemiological studies reported contrasting results
with strong country-specific characteristics due to the different
bioactive compounds contained in coffee in different countries and type
of preparation method used [51], [52] and [53].
Contrasting
with observational studies, a recent meta-analysis of RCT evaluated the
effects of coffee intake on serum lipids in 12 studies conducted on
1017 subjects [54] (Table 1).
On average, drinking coffee for 45 days was associated with an increase
of 8.1 mg/dl (95% CI: 4.5, 11.6) for total cholesterol, 5.4 mg/dl (95%
CI: 1.4, 9.5) for LDL-C, and 12.6 mg/dl (95% CI: 3.5, 12.6) for
triglycerides. Meta-regression analysis also revealed a positive
dose–response relation between coffee intake and total cholesterol,
LDL-C, and triglycerides. However, other more recent studies (thus not
included in the previous meta-analysis) reported poor or little
influence on plasma lipids following acute ingestion of coffee [55] or even a suppression of postprandial hyperlipidemia [56], significant decrease of triglycerides, and increase of HDL-cholesterol [55].
3. Potential beneficial mechanisms of action
3.1. Glucose and insulin metabolism regulation
Despite the acute ingestion of caffeine resulting in a reduction of insulin sensitivity due to decreased glucose storage [57] and [58],
this short-term effect cannot be observed after long-time consumption
of coffee because of an overall impairment of effects of caffeine after
continued intake [59].
Coffee has been reported to be the main contributor of a number of
antioxidant compounds, including some polyphenols such as chlorogenic
acids [60]. This family of polyphenols (mostly caffeic and ferulic acid) demonstrated the ability to affect some metabolic pathways [61] and [62]. In animal models, consumption of chlorogenic acids reduced fasting plasma glucose [63], [64] and [65], increased sensitivity to insulin [66], and slowed the appearance of glucose in circulation after glucose load [67] and [68].
This particular family of molecules showed a specific competitive
inhibition of the glucose-6-phosphate translocase in rat liver
microsomes [69]
an enzyme highly involved in the regulation of homeostasis and blood
glucose levels. At the cellular level, chlorogenic acids activate
adenosine monophosphate-activated protein kinase (AMPK), a sensor and
regulator of cellular energy balance, leading to beneficial metabolic
effects, such as the inhibition of fatty acid synthesis and hepatic
glucose production. Thus, chlorogenic acid by the activation of AMPK may
contribute to lipid and glucose metabolism regulation [70].
Further hypotheses on the mechanism through which chlorogenic acids may
prevent diabetes consist in their capacity to reduce sodium-dependent
glucose transport in brush border membrane vesicles isolated from rat
small intestine [71], and to inhibit α-amylase [72] and [73] and α-glucosidase activity [74] and [75],
two key enzymes responsible for digestion of dietary carbohydrates,
resulting in a reduction of intestinal absorption of glucose.
Together
with phenolic compounds, trigonelline and sex hormone-binding globulin
(SHBG) also demonstrated a protective effect against diabetes [67] and [76]. The vitamin B3
precursor trigonelline has been shown to potentially improve insulin
sensitivity in animal studies by inhibiting dipeptidylpeptidase-4 and
α-glucosidase activities in both plasma and small intestine [77]
and ameliorating the oxidative stress in type 2 diabetic rats
downregulating the gene expressions involved with NADPH oxidase and
mitochondrial electron transfer system [78].
SHBG have been related with type 2 diabetes since membranes of a
variety of cells are able to specifically bind them with high affinity,
and SHBG mediates the steroid-signaling system at the cell membrane
through the SHBG receptors and exerting direct metabolic effects [79].
3.2. Lipid metabolism regulation
It
has been reported that some components present in unfiltered coffee
(i.e., cafestol and kahweol) raise serum lipids, but a clear involvement
in the deposition of LDL-C and/or an oxidation of this lipid fraction
has not been demonstrated. Accordingly, it is still debatable if coffee
consumption can affect lipid metabolism in order to significantly
increase cardiovascular risk [80].
On the contrary, it has been reported that coffee intake increase LDL-C
resistance to oxidative modifications probably as a result of the
incorporation of the phenolic acids in coffee into the cells [81].
An experimental study evaluating the effects of chlorogenic acids on
lipid metabolism in diabetic rats found a significant increase in the
concentrations of plasma and tissue (liver and kidney) lipids,
cholesterol, triglycerides, free fatty acids and phospholipids, and LDL
and very low-density lipoproteins, respectively, and a decrease in the
concentration of HDL [82].
It was demonstrated that their action depended on the capacity to
increase the activity of 3-hydroxy 3-methylglutaryl coenzyme A (HMG-CoA)
reductase in the liver and kidney and a decrease in the activities of
lipoprotein lipase (LPL) and lecithin cholesterol acyl transferase
(LCAT) in the plasma [82].
A
number of epidemiological studies reported a positive association
between coffee consumption and adiponectin levels, an insulin-sensitive
hormone playing a central role in glucose and lipid metabolism, both in
healthy individuals [83], [84], [85] and [86] and in those with metabolic syndrome-related disorders [87] and [88].
These studies remarked the inverse association between coffee
consumption and obesity or visceral fat area. Experimental studies
reported that coffee may play a role in the expression of adipo-R2 gene,
which activate its downstream signaling pathways mainly by activating
AMPK and peroxisome proliferator-activated receptors alpha (PPAR-a) [89].
Coffee polyphenols and melanoidins protected the liver from damage
caused by a hypercaloric diet in an animal model, and this protection
was partially mediated by a reduction in liver inflammation, through
increases of adipo-R2 gene and anti-inflammatory cytokines IL-4 and
IL-10 [90].
3.3. Effects on blood pressure
Despite
caffeine inhibiting phosphodiesterase non-selectively, thereby causing
an accumulation of cAMP, which can mediate a vasoconstrictive response [91], experimental studies reported that an acute increase in blood pressure due to coffee intake develops with rapid tolerance [92] and [93]
and that intravenous caffeine is responsible for the increase in muscle
sympathetic activity and blood pressure in both habitual and
non-habitual coffee drinkers, but coffee intake led to increased blood
pressure only in non-habitual coffee drinkers [94]. Several components of coffee demonstrate anti-hypertensive action [95].
Chlorogenic acids are hypothesized to exert anti-hypertensive effects
by increasing nitric oxide bioavailability and improving endothelial
function, which lead to a reduction of blood pressure [96].
Experimental studies also demonstrated that the depletion in roasted
coffee of hydroxyhydroquinone, a particular fraction of chlorogenic
acid, enhanced the anti-hypertensive effects of chlorogenic acids in a
marginally dose-dependent manner [97].
Moreover, coffee is also rich in blood pressure-lowering minerals
(i.e., potassium and magnesium) that may contribute to its effect on
blood pressure [98].
3.4. Antioxidant activity
Oxidative
stress is heavily involved in metabolism impairment pathways, as well
as in the development of chronic subclinical inflammation that
contribute to chronic disease incidence and progression. The
inflammatory response could be mediated by many factors, such as the
main phenolic compounds of coffee [99].
In particular, chlorogenic acids demonstrated strong antioxidant effect
in a dose–response relationship as a results of the inhibition of the
production of inflammatory mediators [100], [101] and [102], by inhibiting protein tyrosine phosphatase 1B [103] and depressing the expression of pro-inflammatory cytokine genes [104] and [105]. These compounds also demonstrated decreased endothelial dysfunction [106]
by modulating inflammatory NF-κB activation via the redox-related
c-Src/ERK and NIK/IKK pathways via the reduction of oxidative stress [107]. Diterpenes are multitasking molecules that play a role in the regulation of angiogenesis and inflammation processes [108] and [109]. The most studied effects of cafestol regard its capacity to regulate pathological angiogenesis [108].
Kahweol has demonstrated antioxidant properties by inhibiting both
cyclo-oxigenase-2 (COX-2) expression and monocyte chemoattractant
protein-1 (MCP-1) secretion in endothelial cells, key proteins mediating
inflammatory processes [109].
It has been reported that cafestol and kahweol regulate Sp1 target
proteins, which are involved in various biological processes such as
differentiation, metabolism, cell growth, angiogenesis, and apoptosis [110].
Melanoidins, compounds formed during the roasting of coffee beans, have
demonstrated strong antioxidant activity and to significantly inhibit
lipid oxidation [111] and [112].
In an animal model of steatohepatitis, melanoidins protected liver from
damage caused by a high-fat diet by a reduction in hepatic fat
accumulation (through increased fatty acid β-oxidation), systemic and
liver oxidative stress (through the glutathione system), liver
inflammation (through modulation of genes), and expression and
concentrations of proteins and cytokines related to inflammation [90].
Finally, caffeine itself and its metabolites theobromine and xanthine,
have been reported to possess antioxidant properties, such as
DNA-protection through quenching of hydroxyl radical generating systems [113].
4. Controversial effects and future prospective
Besides
the potential beneficial effects of coffee consumption, great attention
should be paid in order to explain its negative effects on human
health. It has been often reported a U-shaped effect of coffee on
several health outcomes [42], [114] and [115],
suggesting that a detrimental effect may occur at higher quantities of
consumption. Moreover, results from epidemiological and experimental
studies are rarely univocal, but rather they are opposite and biased by
methodological limits. Epidemiological studies provide insight into the
long-term effects of coffee consumption but observational evidence
cannot demonstrate causal relationship. Moreover, cross-sectional
studies may have a lack of reliability due to the phenomenon of “reverse
causation”, namely, an adaptation of coffee consumption after
developing the disease. Prospective cohort studies should minimize such
phenomenon, but control over time of coffee consumption may results
difficult and the time distance between the exposure assessment (i.e.,
coffee intake at baseline) and the outcome evaluation may bias results.
Thus, evidence from epidemiological studies is only in part demonstrated
in the experimental setting, and potential confounders (i.e., cigarette
smoking) may affect findings. The randomization process of RCT should,
at least in part, attenuate the effects of confounders theoretically
equally distributed over both intervention and control groups. However,
compared to epidemiological studies, RCT are usually conducted over a
limited period of time. Moreover, the effects follow generally a fixed
dose of coffee (or caffeine) and controlled in a predetermined moment,
thus estimating mostly acute effects of coffee and often not
corresponding to “real-world” coffee drinking. Finally, regarding
experimental studies, most of the data existing is based on in vitro and animal studies, therefore the relevance of findings for the application in humans is still unclear.
5. Conclusion
In
conclusion, in light of the most recent epidemiological and
experimental evidence, coffee consumption seems to be favorably related
with health and to protect by metabolic impairment. Despite the
mechanisms of action being not completely understood, its content in
polyphenols and antioxidant compounds may be countering many of the
negative effects reported in the early researches. Moreover, components
with demonstrated harmful effects (i.e., caffeine and diterpenes) are
nowadays also being reconsidered due to novel discoveries of new
potential positive effects or new hypotheses on their interaction with
metabolism regulation.
Conflict of interest
The authors declare that they have no conflict of interest.
References
- [1]
- Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study
- Lancet, 385 (2015) (2013), pp. 117–171
- [2]
- National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2.7 million participants
- Lancet, 378 (2011), pp. 31–40
- | | |
- [3]
- State of global health—hypertension burden and control
- Blood Press., 21 (Suppl. 1) (2012), pp. 1–2
- | |
- [4]
- Mediterranean diet and cardiovascular risk factors: a systematic review
- Crit. Rev. Food Sci. Nutr., 54 (2014), pp. 593–610
- | |
- [5]
- Impact of lifestyle on metabolic syndrome in apparently healthy people
- Eat. Weight Disord., 19 (2014), pp. 225–232
- | |
- [6]
- Effects of the dietary approach to stop hypertension (DASH) diet on cardiovascular risk factors: a systematic review and meta-analysis
- Br. J. Nutr. (2014), pp. 1–15
- |
- [7]
- A comprehensive meta-analysis on evidence of mediterranean diet and cardiovascular disease: are individual components equal?
- Crit. Rev. Food Sci. Nutr. (2015) [(ahead of Print)]
- [8]
- Protective role of the Mediterranean diet on several cardiovascular risk factors: evidence from Sicily, Southern Italy
- Nutr. Metab. Cardiovasc. Dis., 24 (2014), pp. 370–377
- | | |
- [9]
- A Mediterranean-type diet is associated with better metabolic profile in urban Polish adults: results from the HAPIEE Study
- Metabolism, 64 (2015), pp. 738–746
- | |
- [10]
- Coffee and health: a review of recent human research
- Crit. Rev. Food Sci. Nutr., 46 (2006), pp. 101–123
- | |
- [11]
- Effects of habitual coffee consumption on cardiometabolic disease, cardiovascular health, and all-cause mortality
- J. Am. Coll. Cardiol., 62 (2013), pp. 1043–1051
- | | |
- [12]
- Association of coffee consumption with all-cause and cardiovascular disease mortality
- Mayo Clin. Proc., 88 (2013), pp. 1066–1074
- | | |
- [13]
- Coffee and type 2 diabetes: from beans to beta-cells
- Nutr. Metab. Cardiovasc. Dis., 16 (2006), pp. 69–77
- | | |
- [14]
- Caffeinated and decaffeinated coffee consumption and risk of type 2 diabetes: a systematic review and a dose–response meta-analysis
- Diabetes Care, 37 (2014), pp. 569–586
- | |
- [15]
- Coffee and caffeine intake and incidence of type 2 diabetes mellitus: a meta-analysis of prospective studies
- Eur. J. Nutr., 53 (2014), pp. 25–38
- | |
- [16]
- Coffee to reduce risk of type 2 diabetes? A systematic review
- Curr. Diabetes Rev., 8 (2012), pp. 162–168
- | |
- [17]
- Coffee intake and risk of type 2 diabetes: the multiethnic cohort
- Public Health Nutr. (2013), pp. 1–9
- |
- [18]
- Coffee consumption and risk of chronic disease in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Germany study
- Am. J. Clin. Nutr., 95 (2012), pp. 901–908
- | |
- [19]
- Caffeinated and caffeine-free beverages and risk of type 2 diabetes
- Am. J. Clin. Nutr., 97 (2013), pp. 155–166
- | |
- [20]
- Psychological factors, coffee and risk of diabetes mellitus among middle-aged Japanese: a population-based prospective study in the JPHC study cohort
- Endocr. J., 56 (2009), pp. 459–468
- | |
- [21]
- Consumption of coffee, green tea, oolong tea, black tea, chocolate snacks and the caffeine content in relation to risk of diabetes in Japanese men and women
- Br. J. Nutr., 103 (2010), pp. 453–459
- | |
- [22]
- Coffee consumption and the incidence of type 2 diabetes in men and women with normal glucose tolerance: the Strong Heart Study
- Nutr. Metab. Cardiovasc. Dis., 21 (2011), pp. 418–423
- | | |
- [23]
- Coffee consumption, serum gamma-glutamyltransferase, and glucose tolerance status in middle-aged Japanese men
- Clin. Chem. Lab. Med., 51 (2013), pp. 1233–1239
- |
- [24]
- Coffee and green tea consumption is associated with insulin resistance in Japanese adults
- Metabolism (2013), pp. 400–408
- |
- [25]
- Coffee consumption attenuates short-term fructose-induced liver insulin resistance in healthy men
- Am. J. Clin. Nutr., 99 (2014), pp. 268–275
- | |
- [26]
- Coffee and tea consumption in relation to inflammation and basal glucose metabolism in a multi-ethnic Asian population: a cross-sectional study
- Nutr. J., 10 (2011), p. 61
- [27]
- Associations between the intake of caffeinated and decaffeinated coffee and measures of insulin sensitivity and beta cell function
- Diabetologia, 54 (2011), pp. 320–328
- | |
- [28]
- Systematic review of randomised controlled trials of the effects of caffeine or caffeinated drinks on blood glucose concentrations and insulin sensitivity in people with diabetes mellitus
- J. Hum. Nutr. Diet., 26 (2013), pp. 111–125
- | |
- [29]
- Effects of 16-week consumption of caffeinated and decaffeinated instant coffee on glucose metabolism in a randomized controlled trial
- J. Nutr. Metab., 2012 (2012), p. 207426
- [30]
- Acute effects of light and dark roasted coffee on glucose tolerance: a randomized, controlled crossover trial in healthy volunteers
- Eur. J. Nutr. (2015)
- [31]
- Gender and body mass index modify the effect of increasing amounts of caffeinated coffee on postprandial glucose and insulin concentrations; a randomized, controlled, clinical trial
- Metabolism, 62 (2013), pp. 1099–1106
- | | |
- [32]
- Caffeinated coffee consumption impairs blood glucose homeostasis in response to high and low glycemic index meals in healthy men
- Am. J. Clin. Nutr., 87 (2008), pp. 1254–1261
- |
- [33]
- Decaffeinated coffee and glucose metabolism in young men
- Diabetes Care, 33 (2010), pp. 278–280
- | |
- [34]
- An oral lipid challenge and acute intake of caffeinated coffee additively decrease glucose tolerance in healthy men
- J. Nutr., 141 (2011), pp. 574–581
- | |
- [35]
- Consumption of caffeinated coffee and a high carbohydrate meal affects postprandial metabolism of a subsequent oral glucose tolerance test in young, healthy males
- Br. J. Nutr., 103 (2010), pp. 833–841
- | |
- [36]
- A cross-over study of the acute effects of espresso coffee on glucose tolerance and insulin sensitivity in people with type 2 diabetes mellitus
- Metabolism, 61 (2012), pp. 1231–1237
- | | |
- [37]
- Effects of caffeinated and decaffeinated coffee on biological risk factors for type 2 diabetes: a randomized controlled trial
- Nutr. J., 10 (2011), p. 93
- [38]
- Effects of coffee consumption on subclinical inflammation and other risk factors for type 2 diabetes: a clinical trial
- Am. J. Clin. Nutr., 91 (2010), pp. 950–957
- | |
- [39]
- Habitual coffee consumption and risk of hypertension: a systematic review and meta-analysis of prospective observational studies
- Am. J. Clin. Nutr., 93 (2011), pp. 1212–1219
- | |
- [40]
- The effect of coffee consumption on blood pressure and the development of hypertension: a systematic review and meta-analysis
- J. Hypertens., 30 (2012), pp. 2245–2254
- | |
- [41]
- The effect of coffee on blood pressure and cardiovascular disease in hypertensive individuals: a systematic review and meta-analysis
- Am. J. Clin. Nutr., 94 (2011), pp. 1113–1126
- | |
- [42]
- Blood pressure response to chronic intake of coffee and caffeine: a meta-analysis of randomized controlled trials
- J. Hypertens., 23 (2005), pp. 921–928
- |
- [43]
- Association of daily coffee and tea consumption and metabolic syndrome: results from the Polish arm of the HAPIEE Study
- Eur. J. Nutr. (2014) (ahead of Print)
- [44]
- Coffee consumption and risk of hypertension in the Polish arm of the HAPIEE cohort study
- Eur. J. Clin. Nutr. (2015) [(ahead of print)]
- [45]
- The Tromso Heart Study. Does coffee raise serum cholesterol?
- N. Engl. J. Med., 308 (1983), pp. 1454–1457
- | |
- [46]
- Coffee and tea consumption, dietary fat intake and serum cholesterol concentration of Finnish men and women
- J. Intern. Med., 226 (1989), pp. 127–132
- | |
- [47]
- Coffee consumption and serum cholesterol: an epidemiological study in Belgium
- Int. J. Epidemiol., 17 (1988), pp. 98–104
- [48]
- Coffee and serum cholesterol
- Br. Med. J., 288 (1984), p. 1960
- | |
- [49]
- The cholesterol-raising factor from coffee beans
- Annu. Rev. Nutr., 17 (1997), pp. 305–324
- | |
- [50]
- The effect on serum cholesterol levels of coffee brewed by filtering or boiling
- N. Engl. J. Med., 321 (1989), pp. 1432–1437
- | |
- [51]
- Cholesterol-raising diterpenes in types of coffee commonly consumed in Singapore, Indonesia and India and associations with blood lipids: a survey and cross sectional study
- Nutr. J., 10 (2011), p. 48
- [52]
- Coffee consumption and coronary heart disease in men and women: a prospective cohort study
- Circulation, 113 (2006), pp. 2045–2053
- | |
- [53]
- Factors associated with metabolic syndrome in a Mediterranean population: role of caffeinated beverages
- J. Epidemiol., 24 (2014), pp. 327–333
- | |
- [54]
- The effect of coffee consumption on serum lipids: a meta-analysis of randomized controlled trials
- Eur. J. Clin. Nutr., 66 (2012), pp. 872–877
- | |
- [55]
- The effect of acute cafe latte ingestion on fasting serum lipid levels in healthy individuals
- J. Clin. Lipidol., 7 (2013), pp. 165–168
- | | |
- [56]
- Coffee polyphenols modulate whole-body substrate oxidation and suppress postprandial hyperglycaemia, hyperinsulinaemia and hyperlipidaemia
- Br. J. Nutr., 107 (2012), pp. 1757–1765
- | |
- [57]
- Caffeine-induced impairment of insulin action but not insulin signaling in human skeletal muscle is reduced by exercise
- Diabetes, 51 (2002), pp. 583–590
- | |
- [58]
- Caffeine-induced impairment of glucose tolerance is abolished by beta-adrenergic receptor blockade in humans
- J. Appl. Physiol., 92 (2002) (1985), pp. 2347–2352
- [59]
- Metabolic and exercise endurance effects of coffee and caffeine ingestion
- J. Appl. Physiol., 85 (1998), pp. 883–889
- |
- [60]
- Estimated dietary intake and major food sources of polyphenols in the Polish arm of the HAPIEE Study
- Nutrition, 30 (2014), pp. 1398–1403
- | | |
- [61]
- Isolation and quantification of major chlorogenic acids in three major instant coffee brands and their potential effects on H2O2-induced mitochondrial membrane depolarization and apoptosis in PC-12 cells
- Food Funct., 4 (2013), pp. 1632–1638
- | |
- [62]
- Coffee components and cardiovascular risk: beneficial and detrimental effects
- Int. J. Food Sci. Nutr., 65 (2014), pp. 925–936
- |
- [63]
- Hypoglycemic effect of Cecropia obtusifolia on streptozotocin diabetic rats
- J. Ethnopharmacol., 78 (2001), pp. 145–149
- | |
- [64]
- Chlorogenic acid modifies plasma and liver concentrations of: cholesterol, triacylglycerol, and minerals in (fa/fa) Zucker rats
- J. Nutr. Biochem., 13 (2002), pp. 717–726
- | |
- [65]
- Insulin receptor exon 11 +/− is expressed in Zucker (fa/fa) rats, and chlorogenic acid modifies their plasma insulin and liver protein and DNA
- J. Nutr. Biochem., 17 (2006), pp. 63–71
- | |
- [66]
- Quinides of roasted coffee enhance insulin action in conscious rats
- J. Nutr., 133 (2003), pp. 3529–3532
- [67]
- Acute effects of decaffeinated coffee and the major coffee components chlorogenic acid and trigonelline on glucose tolerance
- Diabetes Care, 32 (2009), pp. 1023–1025
- |
- [68]
- Chlorogenic acid reduces the plasma glucose peak in the oral glucose tolerance test: effects on hepatic glucose release and glycaemia
- Cell Biochem. Funct., 26 (2008), pp. 320–328
- |
- [69]
- Chlorogenic acid and hydroxynitrobenzaldehyde: new inhibitors of hepatic glucose 6-phosphatase
- Arch. Biochem. Biophys., 339 (1997), pp. 315–322
- | |
- [70]
- Anti-diabetic and anti-lipidemic effects of chlorogenic acid are mediated by ampk activation
- Biochem. Pharmacol., 85 (2013), pp. 1341–1351
- | |
- [71]
- Dietary phenolic compounds: inhibition of Na +-dependent d-glucose uptake in rat intestinal brush border membrane vesicles
- J. Nutr., 119 (1989), pp. 1698–1704
- [72]
- Effect of different phenolic compounds on alpha-amylase activity: screening by microplate-reader based kinetic assay
- Pharmazie, 60 (2005), pp. 796–797
- [73]
- Kinetic analysis and mechanism on the inhibition of chlorogenic acid and its components against porcine pancreas alpha-amylase isozymes I and II
- J. Agric. Food Chem., 57 (2009), pp. 9218–9225
- |
- [74]
- Characterization of inhibitors of postprandial hyperglycemia from the leaves of Nerium indicum
- J. Nutr. Sci. Vitaminol., 53 (2007), pp. 166–173
- |
- [75]
- A series of cinnamic acid derivatives and their inhibitory activity on intestinal alpha-glucosidase
- J. Enzyme Inhib. Med. Chem., 24 (2009), pp. 1194–1200
- |
- [76]
- Coffee and caffeine consumption in relation to sex hormone-binding globulin and risk of type 2 diabetes in postmenopausal women
- Diabetes, 60 (2011), pp. 269–275
- |
- [77]
- Experimental diabetes treated with trigonelline: effect on key enzymes related to diabetes and hypertension, beta-cell and liver function
- Mol. Cell. Biochem., 381 (2013), pp. 85–94
- |
- [78]
- Trigonelline ameliorates oxidative stress in type 2 diabetic Goto-Kakizaki rats
- J. Med. Food, 16 (2013), pp. 34–41
- |
- [79]
- Sex hormone-binding globulin and risk of type 2 diabetes in women and men
- N. Engl. J. Med., 361 (2009), pp. 1152–1163
- |
- [80]
- Hydroxyhydroquinone interferes with the chlorogenic acid-induced restoration of endothelial function in spontaneously hypertensive rats
- Am. J. Hypertens., 21 (2008), pp. 23–27
- |
- [81]
- Effects of coffee consumption on oxidative susceptibility of low-density lipoproteins and serum lipid levels in humans
- Biochemistry (Mosc), 69 (2004), pp. 70–74
- [82]
- Antihyperlipidemic effect of chlorogenic acid and tetrahydrocurcumin in rats subjected to diabetogenic agents
- Chem. Biol. Interact., 188 (2010), pp. 643–650
- [83]
- Habitual coffee consumption inversely associated with metabolic syndrome-related biomarkers involving adiponectin
- Nutrition, 29 (2013), pp. 982–987
- [84]
- Association of coffee consumption with serum adiponectin, leptin, inflammation and metabolic markers in Japanese workers: a cross-sectional study
- Nutr. Diabetes, 2 (2012), p. e33
- [85]
- Serum adiponectin concentration in relation to macronutrient and food intake in young Japanese women
- Nutrition, 29 (2013), pp. 1315–1320
- [86]
- Coffee consumption but not green tea consumption is associated with adiponectin levels in Japanese males
- Eur. J. Nutr., 50 (2011), pp. 279–284
- [87]
- Effect of diet and other factors on serum adiponectin concentrations in patients with type 2 diabetes
- Rocz. Panstw. Zakl. Hig., 64 (2013), pp. 61–66
- [88]
- Coffee consumption is associated with higher plasma adiponectin concentrations in women with or without type 2 diabetes: a prospective cohort study
- Diabetes Care, 31 (2008), pp. 504–507
- [89]
- Nutritional and hormonal modulation of adiponectin and its receptors adipoR1 and adipoR2
- Vitam. Horm., 90 (2012), pp. 57–94
- [90]
- Coffee reduces liver damage in a rat model of steatohepatitis: the underlying mechanisms and the role of polyphenols and melanoidins
- Hepatology, 52 (2010), pp. 1652–1661
- [91]
- Caffeine's vascular mechanisms of action
- Int. J. Vasc. Med., 2010 (2010), p. 834060
- [92]
- Tolerance to the humoral and hemodynamic effects of caffeine in man
- J. Clin. Invest., 67 (1981), pp. 1111–1117
- [93]
- Adaptation of blood pressure to continuous heavy coffee drinking in young volunteers. A double-blind crossover study
- Br. J. Clin. Pharmacol., 15 (1983), pp. 701–706
- [94]
- Coffee acutely increases sympathetic nerve activity and blood pressure independently of caffeine content: role of habitual versus nonhabitual drinking
- Circulation, 106 (2002), pp. 2935–2940
- [95]
- Antihypertensive effects and mechanisms of chlorogenic acids
- Hypertens. Res., 35 (2012), pp. 370–374
- [96]
- Ferulic acid restores endothelium-dependent vasodilation in aortas of spontaneously hypertensive rats
- Am. J. Hypertens., 20 (2007), pp. 508–513
- [97]
- Hydroxyhydroquinone-free coffee: a double-blind, randomized controlled dose–response study of blood pressure
- Nutr. Metab. Cardiovasc. Dis., 18 (2008), pp. 408–414
- [98]
- Habitual coffee consumption and blood pressure: an epidemiological perspective
- Vasc. Health Risk Manag., 4 (2008), pp. 963–970
- [99]
- Coffee consumption and human health—beneficial or detrimental?—Mechanisms for effects of coffee consumption on different risk factors for cardiovascular disease and type 2 diabetes mellitus
- Mol. Nutr. Food Res., 49 (2005), pp. 274–284
- [100]
- The polyphenol chlorogenic acid inhibits staphylococcal exotoxin-induced inflammatory cytokines and chemokines
- Immunopharmacol. Immunotoxicol., 24 (2002), pp. 113–119

- [101]
- Evaluation of the anti-inflammatory, analgesic and antipyretic activities of the natural polyphenol chlorogenic acid
- Biol. Pharm. Bull., 29 (2006), pp. 2236–2240
- [102]
- In vitro antioxidant activity of coffee compounds and their metabolites
- J. Agric. Food. Chem., 55 (2007), pp. 6962–6969
- [103]
- Inhibition of protein tyrosine phosphatase 1B and regulation of insulin signalling markers by caffeoyl derivatives of chicory (Cichorium intybus) salad leaves
- Br. J. Nutr., 104 (2010), pp. 813–823
- [104]
- Coffee and caffeine improve insulin sensitivity and glucose tolerance in C57BL/6J mice fed a high-fat diet
- Biosci. Biotechnol. Biochem., 75 (2011), pp. 2309–2315
- [105]
- Effects of coffee on inflammatory cytokine gene expression in mice fed high-fat diets
- J. Agric. Food Chem., 57 (2009), pp. 11100–11105
- [106]
- Coffee consumption and markers of inflammation and endothelial dysfunction in healthy and diabetic women
- Am. J. Clin. Nutr., 84 (2006), pp. 888–893
- [107]
- Caffeic acid regulates LPS-induced NF-kappaB activation through NIK/IKK and c-src/ERK signaling pathways in endothelial cells
- Arch. Pharm. Res. (2013)
- [108]
- Antiangiogenic properties of cafestol, a coffee diterpene, in human umbilical vein endothelial cells
- Biochem. Biophys. Res. Commun., 421 (2012), pp. 567–571
- [109]
- Anti-angiogenic and anti-inflammatory properties of kahweol, a coffee diterpene
- PLoS One, 6 (2011), p. e23407
- [110]
- Natural diterpenes from coffee, cafestol and kahweol induce apoptosis through regulation of specificity protein 1 expression in human malignant pleural mesothelioma
- J. Biomed. Sci., 19 (2012), p. 60
- [111]
- Chemical characterization and antioxidant properties of coffee melanoidins
- J. Agric. Food Chem., 50 (2002), pp. 6527–6533
- [112]
- Antioxidative activity of the blue pigment formed in a d-xylose-glycine reaction system
- Biosci. Biotechnol. Biochem., 67 (2003), pp. 54–59
- [113]
- Antioxidant and prooxidant properties of caffeine, theobromine and xanthine
- Med. Sci. Monit., 9 (2003), pp. BR325–BR330
- [114]
- Non-alcoholic beverage and caffeine consumption and mortality: the Leisure World Cohort Study
- Prev. Med., 44 (2007), pp. 305–310
- [115]
- Consumption of coffee is associated with reduced risk of death attributed to inflammatory and cardiovascular diseases in the Iowa Women's health study
- Am. J. Clin. Nutr., 83 (2006), pp. 1039–1046
© 2016 The Authors. Published by Elsevier GmbH on behalf of Society of Nutrition and Food Science e.V.
Subscribe to:
Posts (Atom)